Lecture 4: Factors in Alveolar Ventilation
Slide 1
- This lecture examines the factors that contribute to alveolar ventilation and the equations used to calculate gas transport and exchange at the pulmonary level.
- Topics include the Fick principle for oxygen transport by convection, Fick’s law of diffusion across the blood-gas barrier, the diffusion capacity of the lungs, and the clinical alveolar ventilation equations.
Slide 2
Overview and Learning Objectives
- Overview topics: Fundamentals of gas exchange and the oxygen supply cascade; lung structure and function; ventilation at rest and responses to exercise.
- Learning objectives:
- Review factors that contribute to alveolar ventilation.
- Use the Fick principle to calculate gas transport by ventilatory convection.
- Use Fick’s law of diffusion to calculate gas transport from alveoli to blood.
- Discuss conditions that may lead to pulmonary limitations in gas exchange.
Slide 3
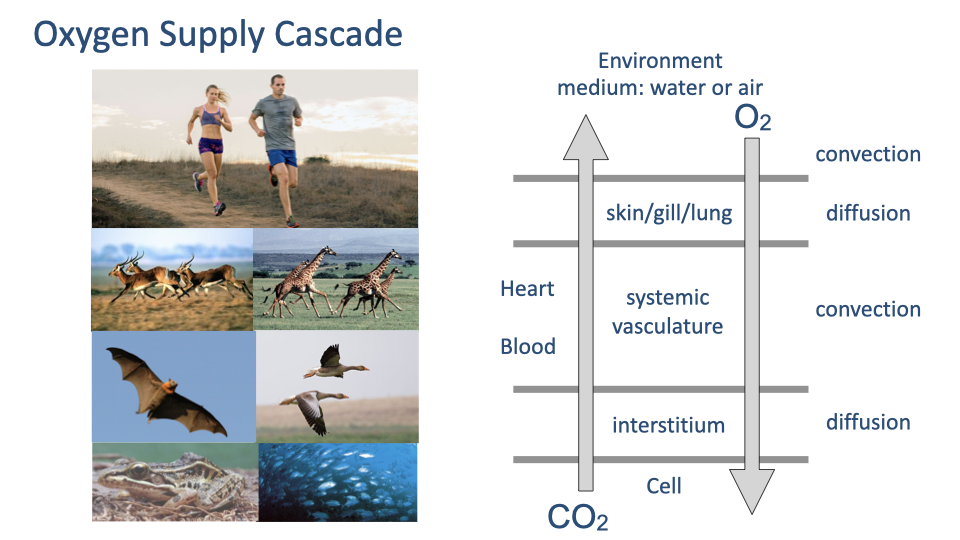
Oxygen Supply Cascade Review
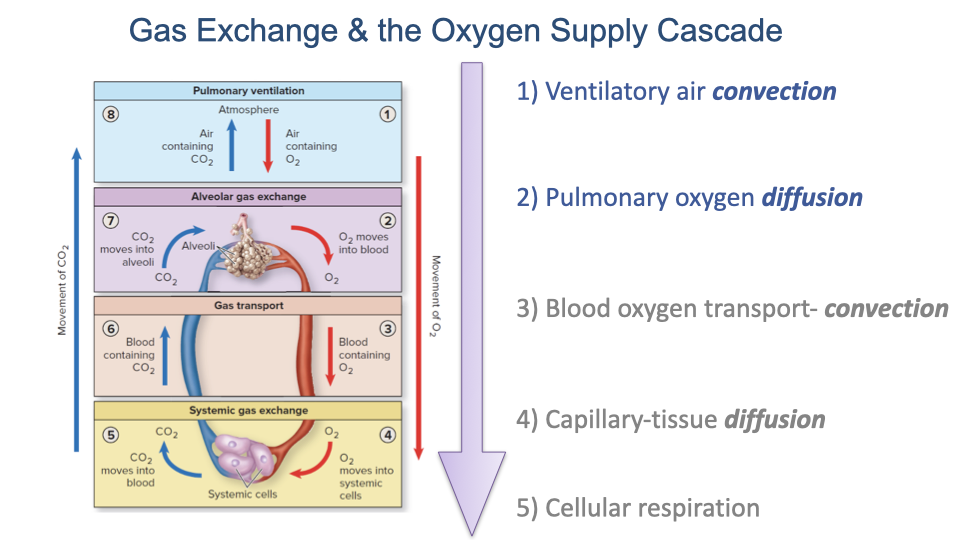
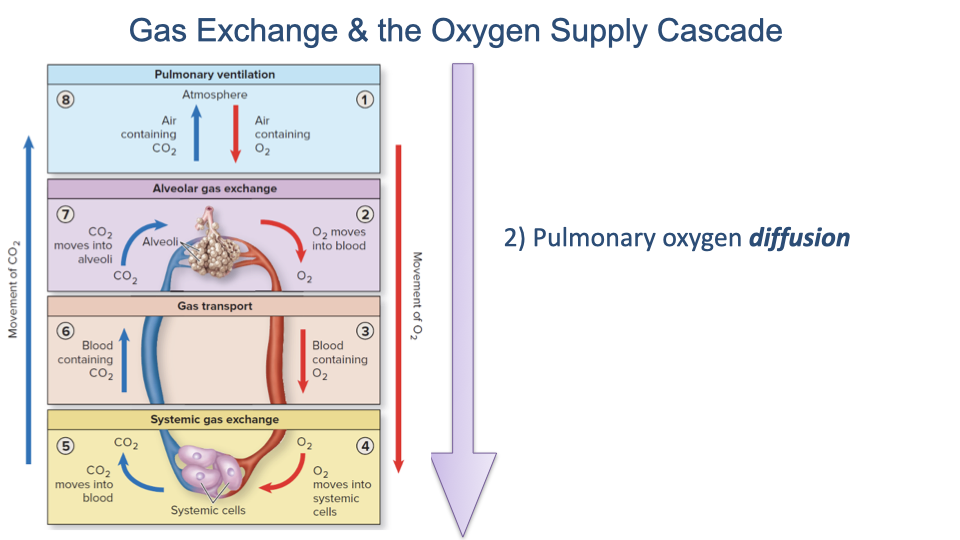
- The oxygen supply cascade traces the progressive decrease in PO2 from the environment to the mitochondria through alternating convection and diffusion steps.
- Convection (bulk flow) moves gases over long distances: ventilation moves air into the lungs, and the circulatory system transports O2 in the blood.
- Diffusion moves gases across thin barriers at the lung surface and at tissue capillaries.
- CO2 flows in the reverse direction, from cells back to the environment.
- This lecture focuses on building up the governing equations for pulmonary convection and diffusion.
Slide 4
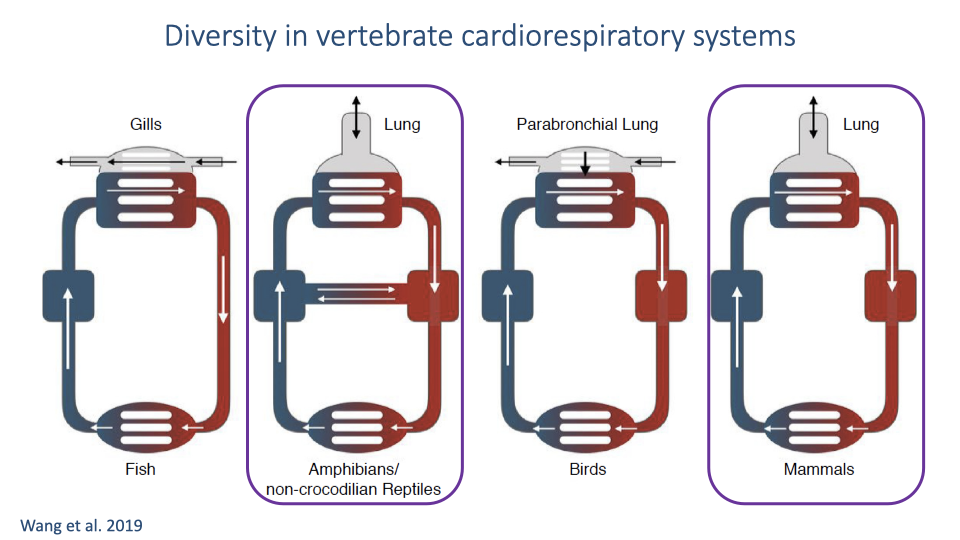
Diversity in Vertebrate Cardiorespiratory Systems
- Vertebrate gas exchange systems vary widely in design, but all must accomplish the same fundamental task of exchanging O2 and CO2.
- Fish use gills with countercurrent exchange (water and blood flow in opposite directions).
- Birds have parabronchial lungs with unidirectional airflow and cross-current exchange – no anatomical dead space.
- Mammals, amphibians and non-crocodilian reptiles use tidal ventilation where air moves in and out through the same passages, creating a “pool” exchange system with anatomical dead space.
- The human tidal ventilation system means not all air is refreshed on each breath, and alveolar gas composition varies depending on metabolic rate, tidal volumes, and breathing frequency.
Slide 5
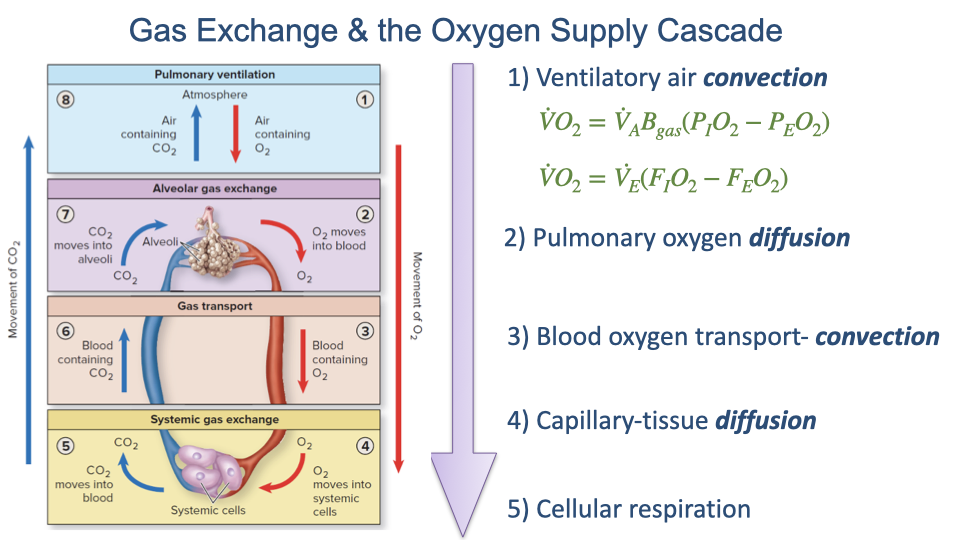
Gas Exchange Steps in the Oxygen Supply Cascade
- The oxygen supply cascade consists of five sequential steps:
- Ventilatory air convection – moving air into the lungs
- Pulmonary oxygen diffusion – O2 crosses the blood-gas barrier
- Blood oxygen transport – convection via the circulatory system
- Capillary-tissue diffusion – O2 crosses into tissues
- Cellular respiration – O2 used by mitochondria
- This lecture builds the equations governing Steps 1 and 2, which together determine pulmonary gas exchange.
Slide 6
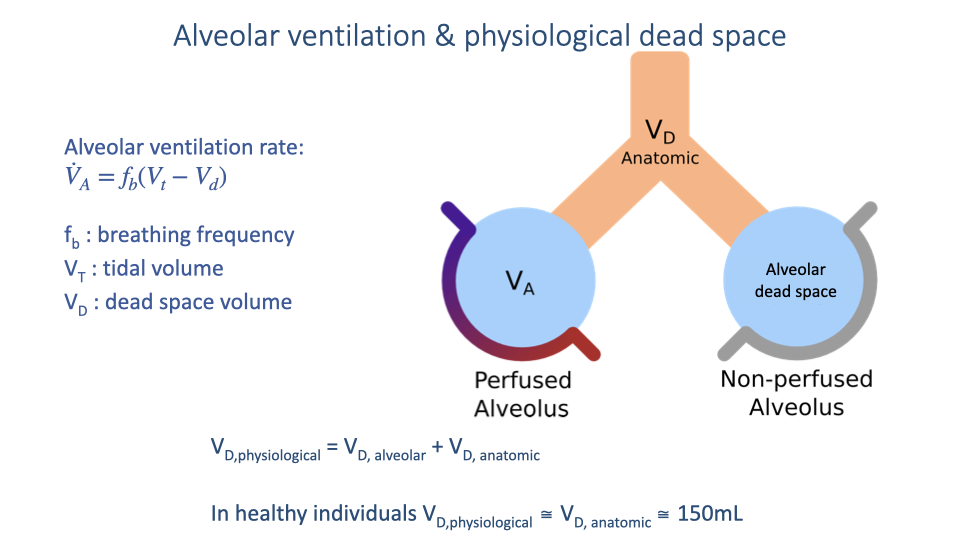
Review of Alveolar Ventilation and Physiological Dead Space
- The alveolar ventilation rate is defined by:
- Where $f_b$ is breathing frequency, $V_T$ is tidal volume, and $V_D$ is dead space volume.
- Physiological dead space has two components:
- Anatomic dead space: the volume of the conducting airways (~150 mL in healthy adults).
- Alveolar dead space: alveoli that are ventilated but not perfused with capillary blood, so they do not participate in gas exchange.
- In healthy individuals, physiological dead space is approximately equal to anatomic dead space (~150 mL), because nearly all alveoli are well perfused.
Slide 7
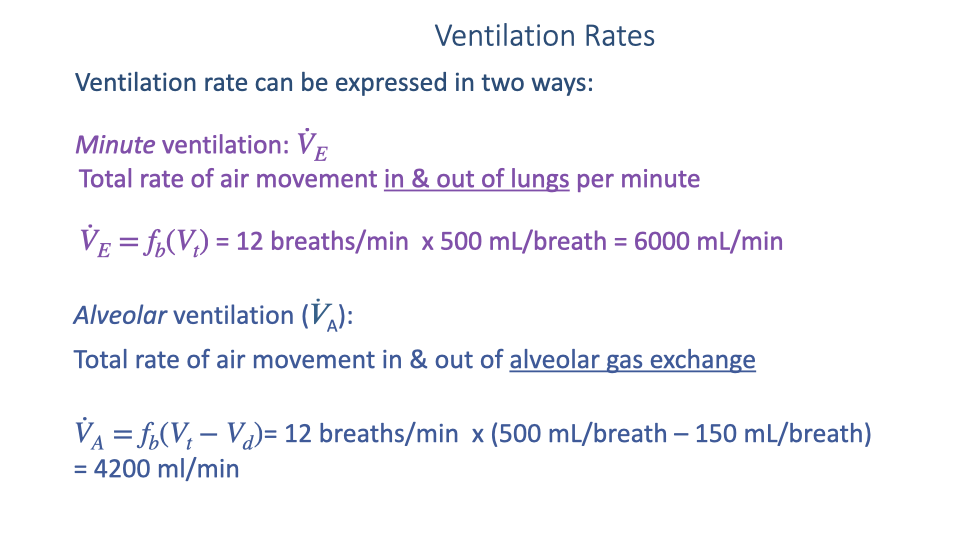
Ventilation Rates: Minute vs. Alveolar
- Minute ventilation ($\dot{V}_E$): the total rate of air movement in and out of the lungs per minute.
- Alveolar ventilation ($\dot{V}_A$): the rate of air movement in and out of the alveolar gas exchange surfaces, accounting for dead space.
- Alveolar ventilation is the physiologically relevant measure for gas exchange because only air reaching perfused alveoli participates in O2 and CO2 exchange.
- The difference (1800 mL/min in this example) represents dead space ventilation.
Slide 8
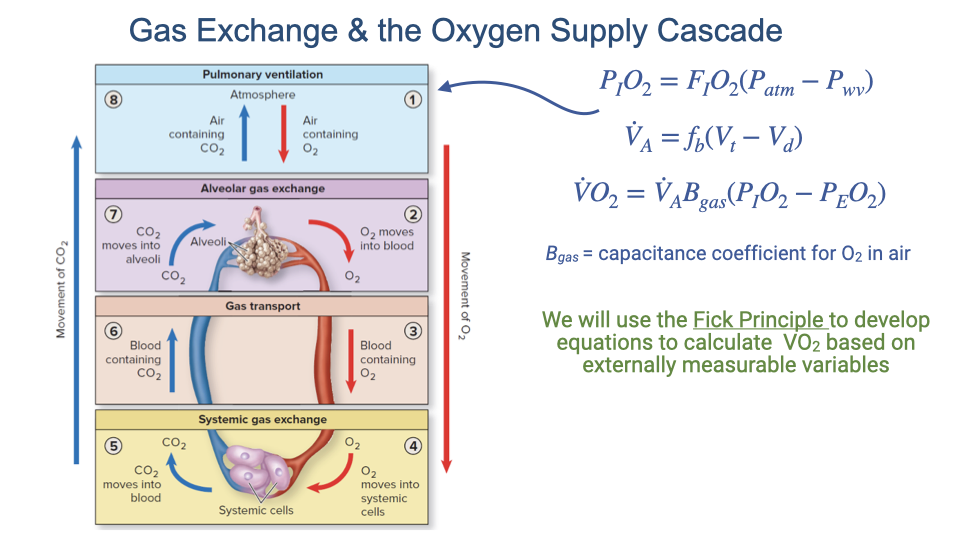
Building the Oxygen Transport Equations
- The equations developed so far for Step 1 (ventilatory air convection) include:
- $\beta_{gO_2}$ is the capacitance coefficient for O2 in air.
- The third equation calculates $\dot{V}$O2 but relies on internal variables (alveolar partial pressures) that are difficult to measure directly.
- The Fick principle will be used to reformulate these equations in terms of externally measurable quantities.
Slide 9
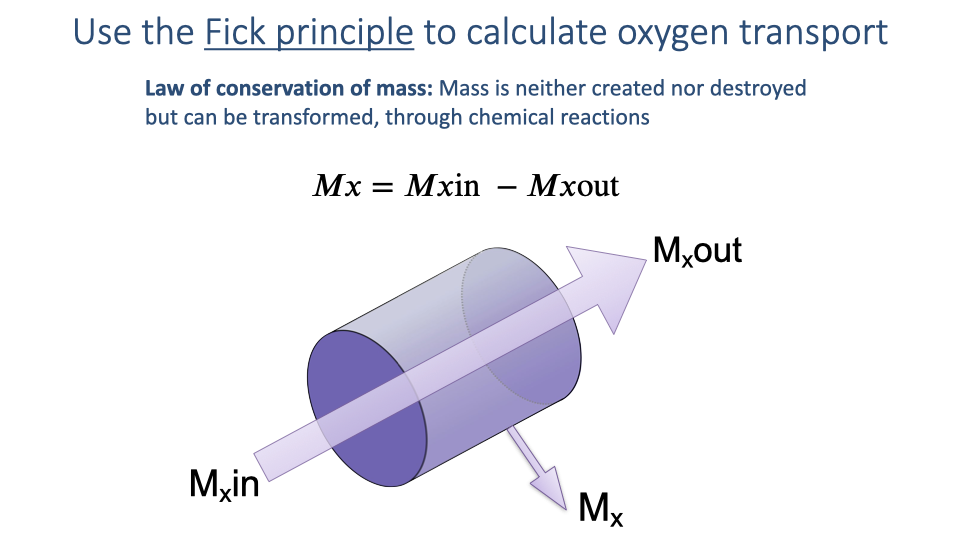
The Fick Principle: Conservation of Mass
- The Fick principle is based on the law of conservation of mass: mass is neither created nor destroyed but can be transformed through chemical reactions.
- For any substance $x$ flowing through a system:
- The amount of substance taken up (or released) by the system equals the difference between what enters and what leaves.
- Applied to oxygen: the mass of O2 taken up by the body equals the difference between O2 in the inhaled air and O2 in the exhaled air.
- This principle allows measurement of gas exchange using external (non-invasive) measurements at the mouth, rather than requiring internal probes.
Slide 10
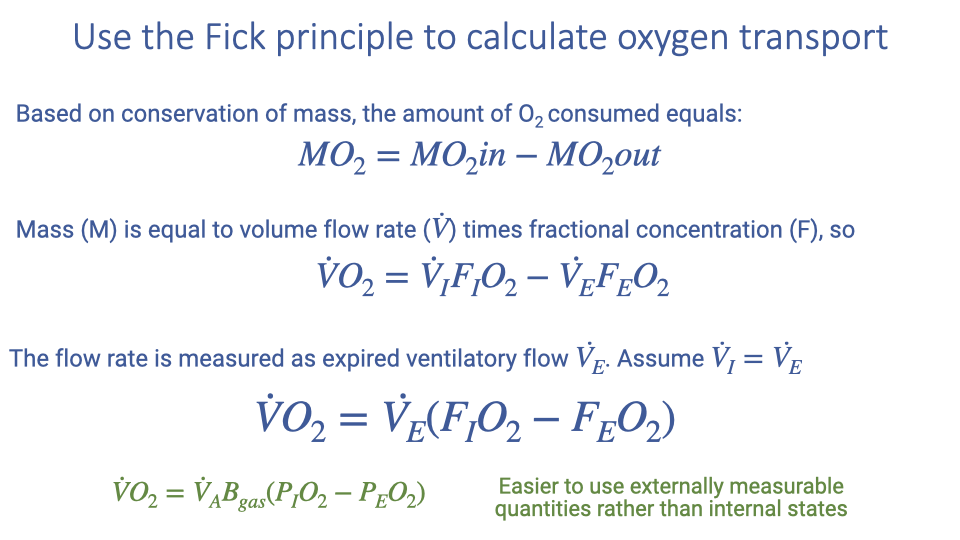
Applying the Fick Principle to Oxygen Transport
- Based on conservation of mass, the rate of O2 consumption equals:
- Since mass equals volume flow rate times fractional concentration:
- Where $\dot{V}_I$ is the inspired ventilatory flow rate, $\dot{V}_E$ is the expired ventilatory flow rate, $F_IO_2$ is the fractional concentration of inspired O2, and $F_EO_2$ is the fractional concentration of expired O2.
- Because $\dot{V}_I \approx \dot{V}_E$, the equation simplifies to:
- This simplified form uses externally measurable quantities (exhaled flow rate and gas concentrations) rather than internal alveolar states, making it practical for laboratory and clinical use.
- Typically, only a few percent of inhaled O2 is extracted per breath (e.g., from ~21% to ~19%).
Slide 11
Human VO2 Max Testing
- $\dot{V}$O2 max is a central measure of maximal aerobic capacity and athletic performance, widely used in exercise physiology and sports science.
- Modern metabolic measurement systems use the Fick-principle-based equations to measure O2 consumption non-invasively.
- The subject wears a sealed mask over the nose and mouth; the system measures the expired flow rate ($\dot{V}_E$) and the fractional concentrations of O2 and CO2 in the exhaled air.
- Earlier systems required bulky laboratory carts, but portable systems are now available, enabling metabolic rate measurement during diverse exercise conditions in the field.
Slide 12
Summary: Ventilatory Convection Equations
- Two equivalent forms for calculating $\dot{V}$O2 at Step 1 have been developed:
- Internal variables form: $\dot{V}O_2 = \dot{V}_A \times \beta_{gO_2} \times (P_IO_2 - P_EO_2)$ — requires measuring alveolar partial pressures (impractical).
- External variables form: $\dot{V}O_2 = \dot{V}_E \times (F_IO_2 - F_EO_2)$ — uses expired ventilation rate and gas fractions (practical, non-invasive).
- The Fick-principle-based external equation is the foundation for all modern respiratory gas exchange measurement in exercise physiology and clinical settings.
Slide 13
Step 2: Pulmonary Oxygen Diffusion
- After air reaches the alveoli by convection (Step 1), oxygen must cross the blood-gas barrier by diffusion (Step 2).
- The rate of diffusion across the alveolar membrane is the next critical factor determining how much O2 enters the blood.
- Fick’s law of diffusion provides the governing equation for this step.
Slide 14
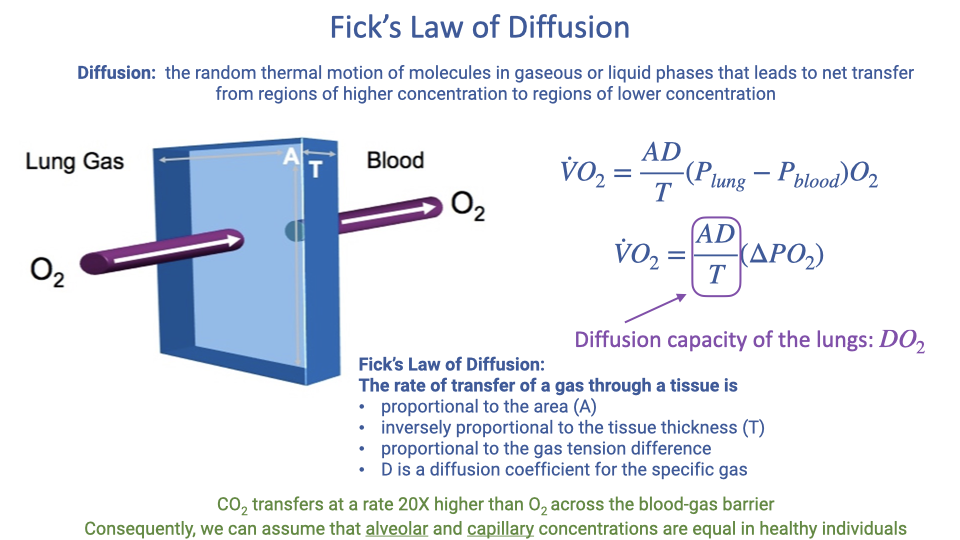
Fick’s Law of Diffusion
- Diffusion is the random thermal motion of molecules in gaseous or liquid phases, resulting in net transfer from regions of higher concentration to regions of lower concentration until equilibrium is reached.
- Fick’s law of diffusion for gas transfer across a tissue barrier:
- Where:
- $A$ = surface area of the gas exchange membrane
- $D$ = diffusion coefficient for the specific gas
- $\Delta P_{O_2}$ = partial pressure difference across the barrier (PAO2 - PaO2)
- $T$ = thickness of the tissue barrier
- The diffusion rate is:
- Proportional to surface area ($A$)
- Proportional to the partial pressure gradient ($\Delta P_{O_2}$)
- Inversely proportional to barrier thickness ($T$)
- $D$ differs between gases: CO2 diffuses approximately 20 times faster than O2 across the blood-gas barrier, meaning CO2 transfer is nearly instantaneous while O2 transfer may be rate-limiting.
Slide 15
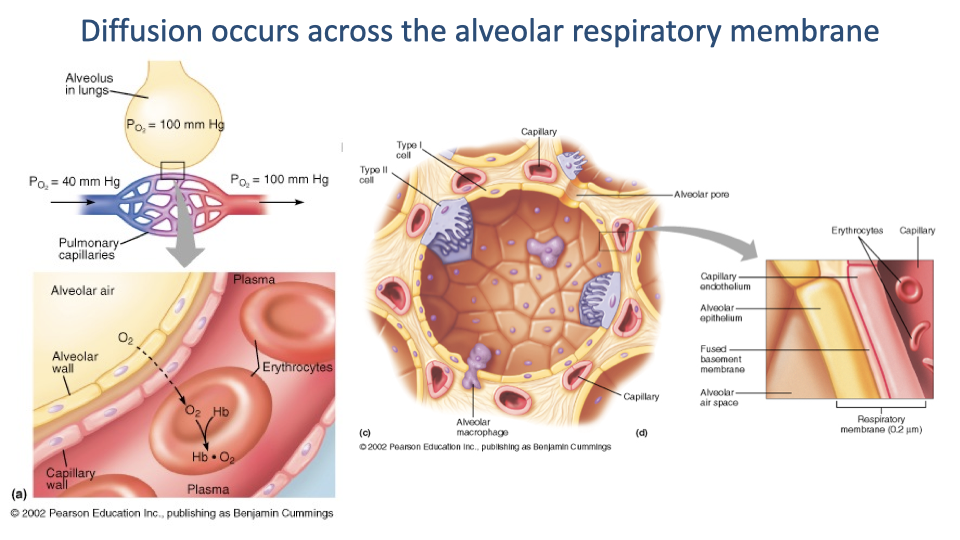
The Alveolar Respiratory Membrane
- Gas exchange occurs across the alveolar respiratory membrane, which separates alveolar air from capillary blood.
- The membrane consists of multiple thin layers: the alveolar epithelium, fused basement membranes, and the capillary endothelium, with a total thickness of approximately 0.2 micrometers.
- Typical partial pressure values at rest:
- PO2 in the alveolus: ~104 mmHg; in deoxygenated blood: ~40 mmHg (gradient of ~64 mmHg drives O2 into blood)
- PCO2 in the blood: ~45 mmHg; in the alveolus: ~40 mmHg (gradient of ~5 mmHg drives CO2 into alveolus)
- Despite the smaller CO2 gradient, CO2 diffuses adequately because its diffusion coefficient is ~20 times that of O2.
Slide 16
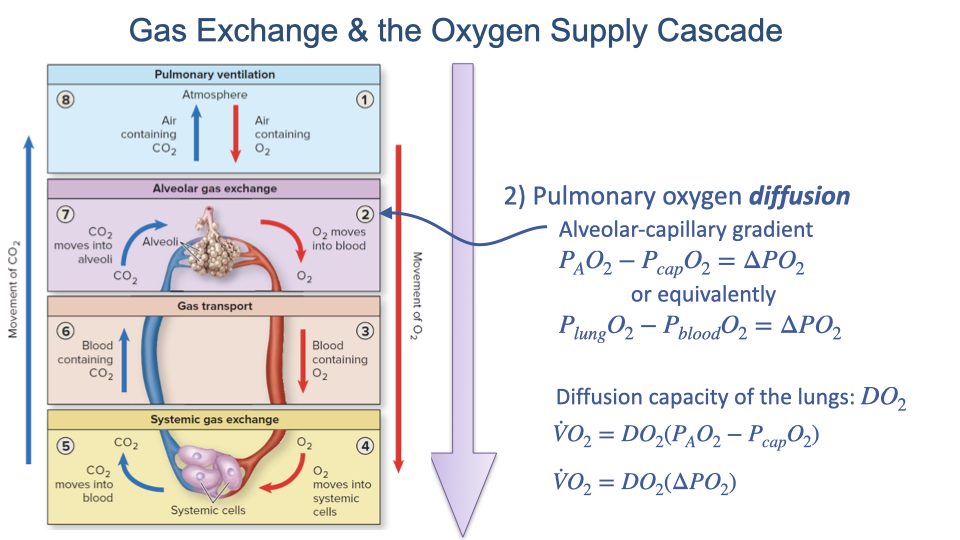
Diffusion Capacity of the Lungs
- The partial pressure gradient driving pulmonary O2 diffusion is:
- The structural factors in Fick’s law (surface area, diffusion coefficient, and barrier thickness) are combined into a single term called the diffusion capacity of the lungs (DLO2):
- The simplified diffusion equation then becomes:
- This formulation highlights the two key determinants of pulmonary O2 transfer:
- Diffusion capacity (DLO2) – determined by lung structure (surface area, membrane thickness, gas properties)
- Partial pressure gradient ($\Delta P_{O_2}$) – determined by alveolar ventilation, inspired O2, and blood perfusion
Slide 17
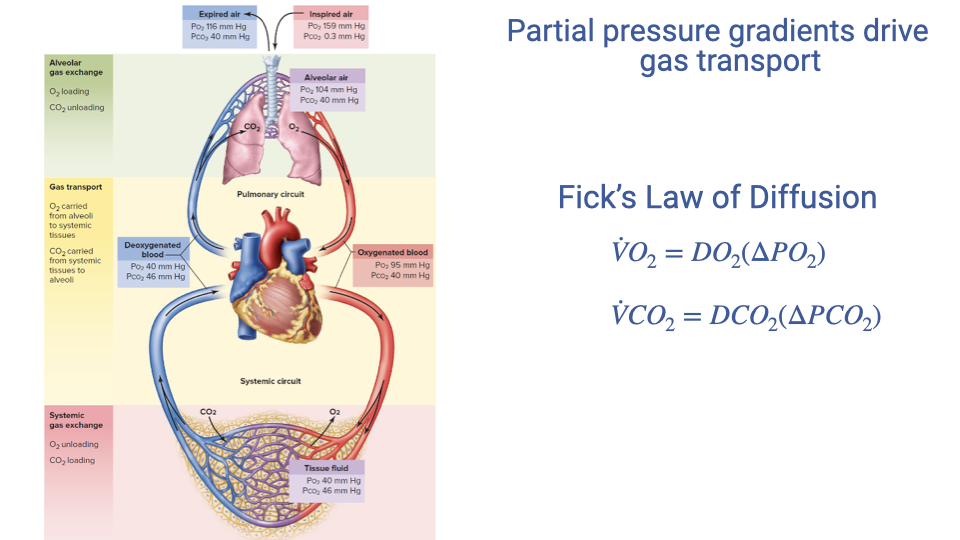
Partial Pressure Gradients Drive Gas Transport
- The same diffusion principle applies to both O2 and CO2:
- O2 diffuses from the alveoli into the pulmonary capillary blood (down the PO2 gradient).
- CO2 diffuses from the blood into the alveoli (down the PCO2 gradient).
- Because CO2 has a much higher diffusion coefficient, equilibrium between blood and alveolar CO2 is achieved nearly instantaneously. O2 equilibration takes longer and can become a limiting factor under certain conditions (e.g., high-intensity exercise, altitude).
Slide 18
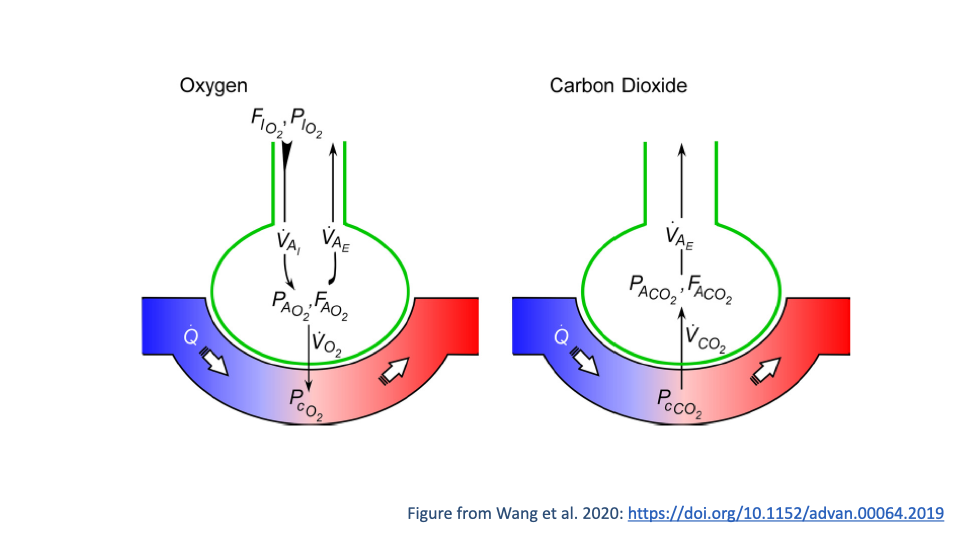
Integrated Model of Alveolar Gas Exchange
- This schematic integrates the convective and diffusive components of pulmonary gas exchange for both O2 and CO2.
- Oxygen (left panel):
- Inspired air with fractional concentration $F_IO_2$ and partial pressure $P_IO_2$ enters the alveolus.
- Alveolar ventilation ($\dot{V}_A$) refreshes alveolar gas.
- O2 diffuses across the membrane into the capillary blood (perfusion $\dot{Q}$), driven by the gradient between PAO2 and PcO2.
- Carbon dioxide (right panel):
- CO2 diffuses from blood (PcCO2) into the alveolus.
- Exhaled ventilation removes CO2 from the lung.
- Ventilation, perfusion, and diffusion all influence the alveolar partial pressures of both gases.
Slide 19
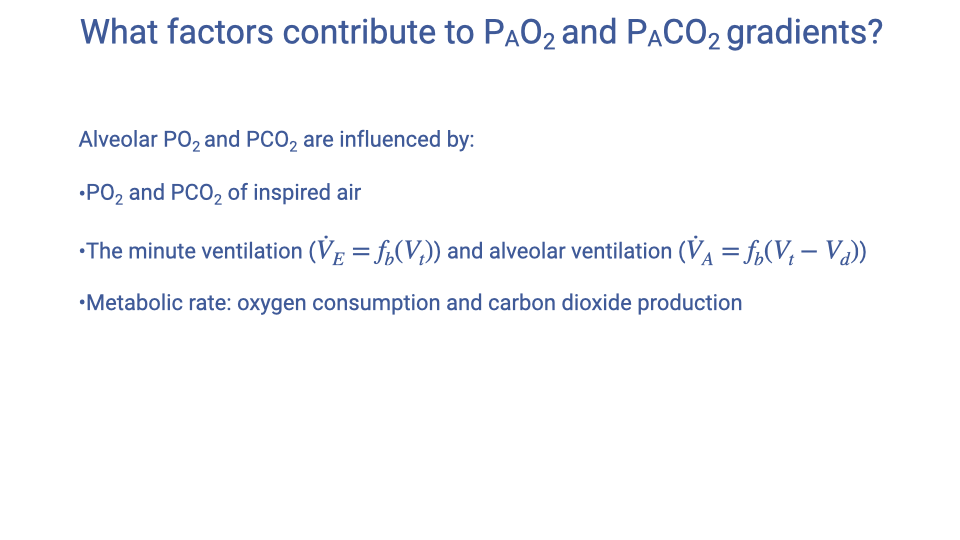
Factors Contributing to Alveolar Partial Pressure Gradients
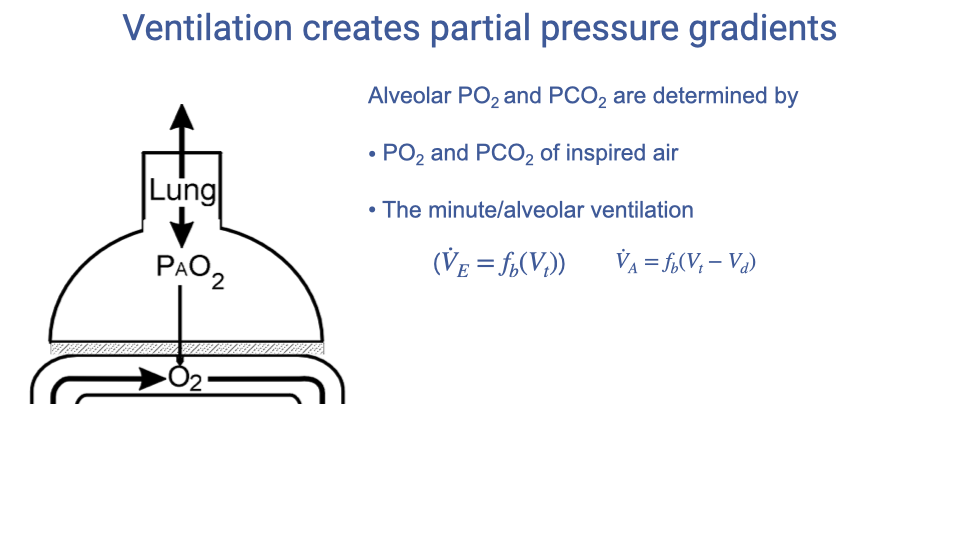
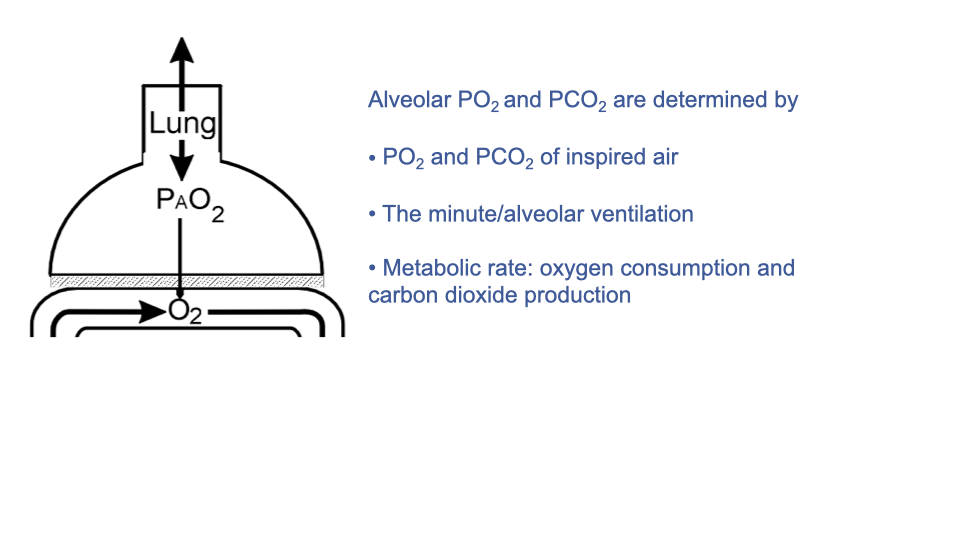
- Three primary factors influence alveolar PO2 and PCO2:
- PO2 and PCO2 of the inspired air – determined primarily by altitude and environmental conditions.
- Minute ventilation ($\dot{V}_E = f_b \times V_T$) and alveolar ventilation ($\dot{V}_A = f_b \times (V_T - V_D)$) – how much fresh air reaches the gas exchange surfaces.
- Metabolic rate – the rate of O2 consumption and CO2 production by the tissues, which creates the demand for gas exchange.
- Altering any of these three factors changes the gas composition in the alveoli and therefore the partial pressure gradients driving diffusion. We walk through each of these factors over the next several slides.
Slide 20
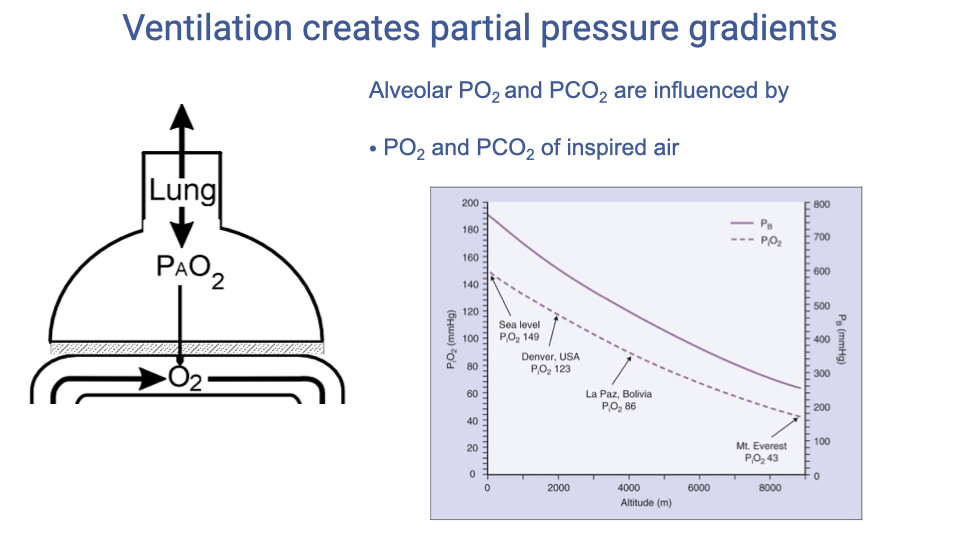
Factor 1: Inspired Air Composition
- The partial pressure of O2 in the inspired air (PIO2) sets the upper limit of alveolar PO2.
- At high altitude, barometric pressure decreases, reducing PIO2 and thereby lowering alveolar PO2.
- In enclosed or poorly ventilated spaces, exhaled CO2 can accumulate in the ambient air, which may also alter inspired gas composition.
- Under normal sea-level conditions, the inspired PO2 is approximately 149 mmHg and is not typically a limiting factor.
Slide 21
Factor 2: Minute and Alveolar Ventilation
- The rate at which fresh air is delivered to the alveoli directly determines how well alveolar gases are renewed.
- Minute ventilation ($\dot{V}_E = f_b \times V_T$) is the total volume of air moved per minute.
- Alveolar ventilation ($\dot{V}_A = f_b \times (V_T - V_D)$) is the fraction that actually reaches gas exchange surfaces.
- Increasing ventilation brings more fresh air into the alveoli, raising alveolar PO2 and lowering alveolar PCO2.
- Decreasing ventilation has the opposite effect, allowing CO2 to accumulate and O2 to drop.
Slide 22
Effects of Ventilation Rate on Lung Gases
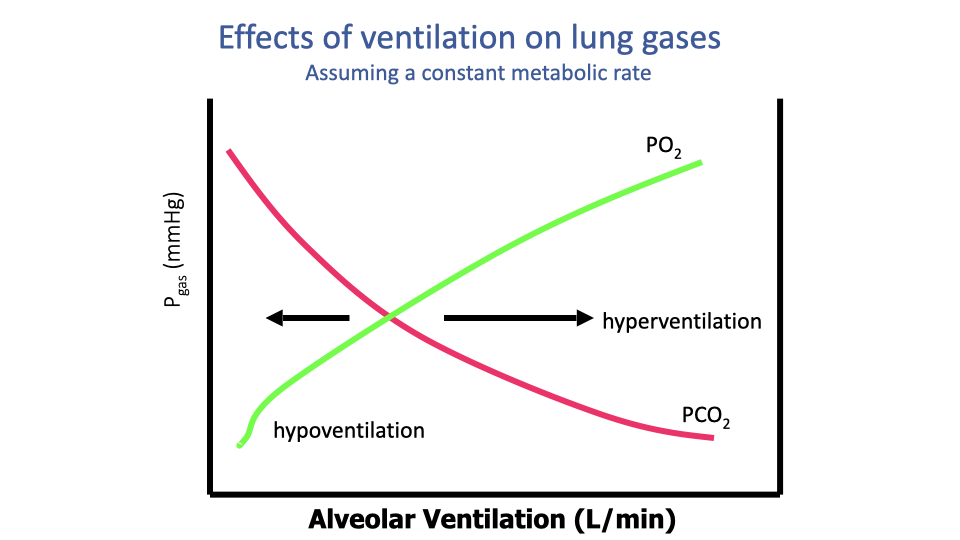
- At a constant metabolic rate, changing the alveolar ventilation rate alters the gas mixture in the lungs:
- Increasing ventilation raises alveolar PO2 and lowers alveolar PCO2 (more fresh air dilutes CO2 and replenishes O2).
- Decreasing ventilation lowers alveolar PO2 and raises alveolar PCO2.
- Hyperventilation (breathing too fast relative to metabolic demand) blows off CO2 faster than it is produced, lowering blood CO2 and raising blood pH. This disrupts acid-base balance and can cause dizziness and, if prolonged, loss of consciousness.
- Hypoventilation (breathing too slowly) causes CO2 accumulation and O2 depletion, leading to poor gas exchange. It is seen clinically with respiratory depression from drugs, sedation, or obstructive pulmonary diseases.
- Normal breathing is regulated by homeostatic mechanisms to maintain appropriate alveolar gas concentrations for the current metabolic demand.
Slide 23
Factor 3: Metabolic Rate
- The third factor influencing alveolar gas composition is the metabolic rate of the tissues – the rate of O2 consumption ($\dot{V}$O2) and CO2 production ($\dot{V}$CO2).
- As metabolic rate increases (e.g., during exercise), tissues consume more O2 and produce more CO2.
- If ventilation does not increase proportionally, alveolar PO2 drops and alveolar PCO2 rises.
- Under normal conditions, homeostatic regulation rapidly adjusts breathing rate and depth in response to changes in metabolic rate, maintaining appropriate alveolar gas composition.
Slide 24
Effects of Metabolic Rate on Lung Gases
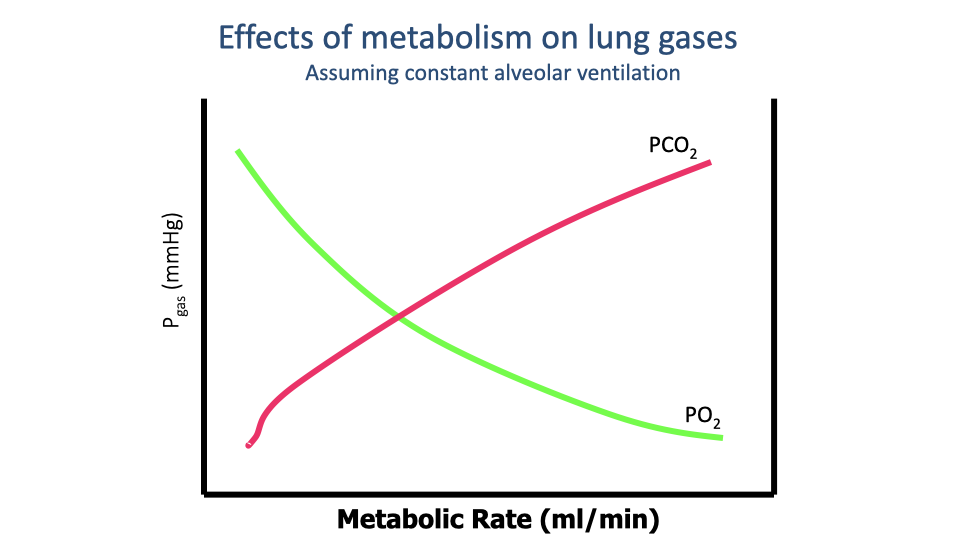
- At constant alveolar ventilation, increasing metabolic rate changes alveolar gas composition:
- PO2 decreases because O2 is consumed by tissues faster than ventilation can replenish it.
- PCO2 increases because CO2 is produced faster than ventilation can remove it.
- This is a hypothetical scenario – in practice, ventilation rate increases rapidly when exercise begins, driven by homeostatic regulation.
- The relationship illustrates why ventilation and metabolism must be closely matched: a mismatch in either direction disrupts the alveolar gas environment and can impair gas exchange.
- The respiratory exchange ratio (R = $\dot{V}$CO2 / $\dot{V}$O2) reflects the balance between CO2 production and O2 consumption and depends on the metabolic substrates being used.
Slide 25
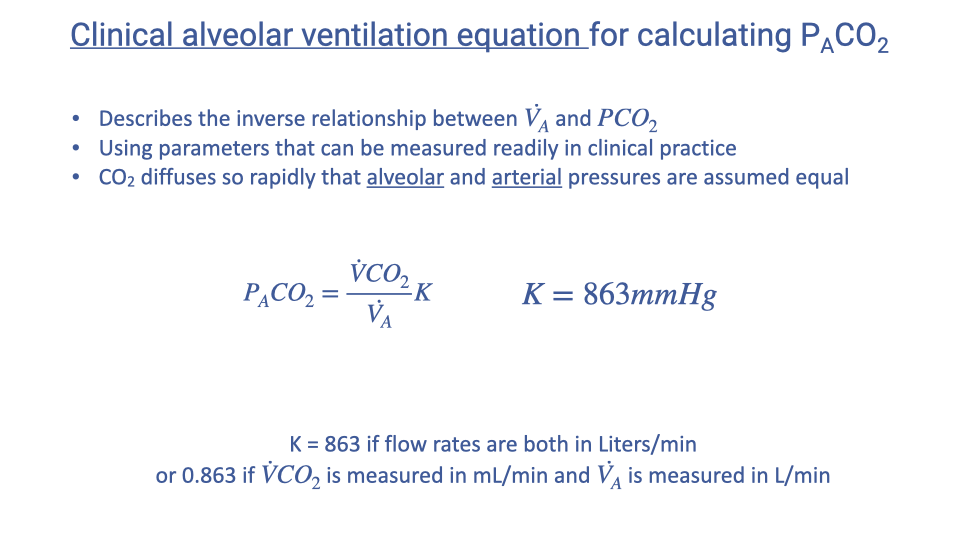
Clinical Alveolar Ventilation Equation for PACO2
- The clinical alveolar ventilation equation describes the inverse relationship between alveolar ventilation rate and alveolar CO2 partial pressure:
- Where $K = 863$ mmHg (when both flow rates are in L/min at BTPS/STPD conditions).
- If $\dot{V}$CO2 is in mL/min and $\dot{V}_A$ is in L/min, then $K = 0.863$.
- Because CO2 diffuses so rapidly across the blood-gas barrier, alveolar PCO2 and arterial PCO2 are assumed to be equal (PACO2 $\approx$ PaCO2).
- This equation uses parameters that can be readily measured with spirometry in the clinic: exhaled CO2 flow rate and alveolar ventilation rate.
Slide 26
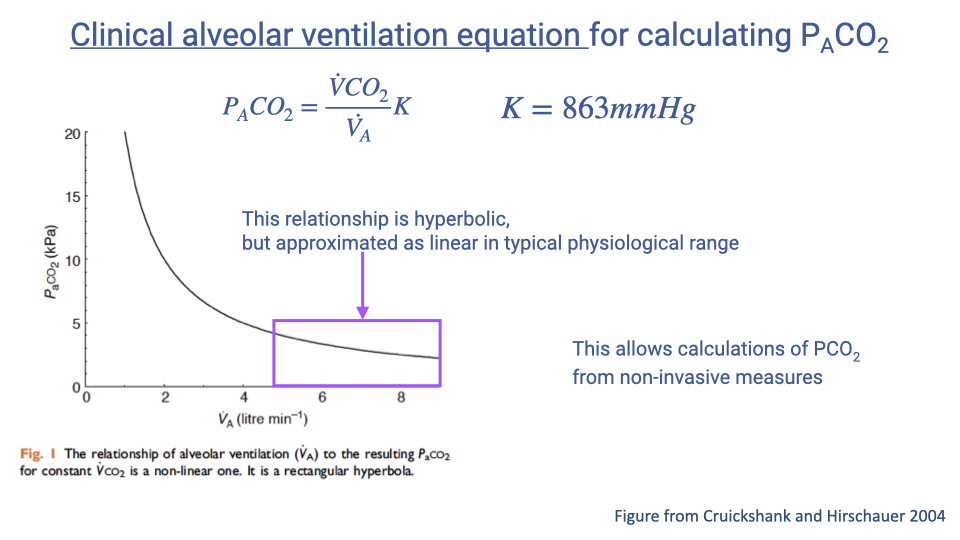
PACO2 vs. Alveolar Ventilation: Clinical Approximation
- The relationship between alveolar ventilation and PACO2 is mathematically hyperbolic (an inverse relationship).
- However, within the clinically relevant physiological range, it is approximated as linear, which simplifies clinical calculations.
- This approximation allows clinicians to estimate alveolar (and arterial) CO2 levels from non-invasive spirometric measurements.
- The clinical significance is that changes in ventilation rate predictably affect blood CO2, making this equation valuable for diagnosing and managing ventilatory disorders.
Slide 27
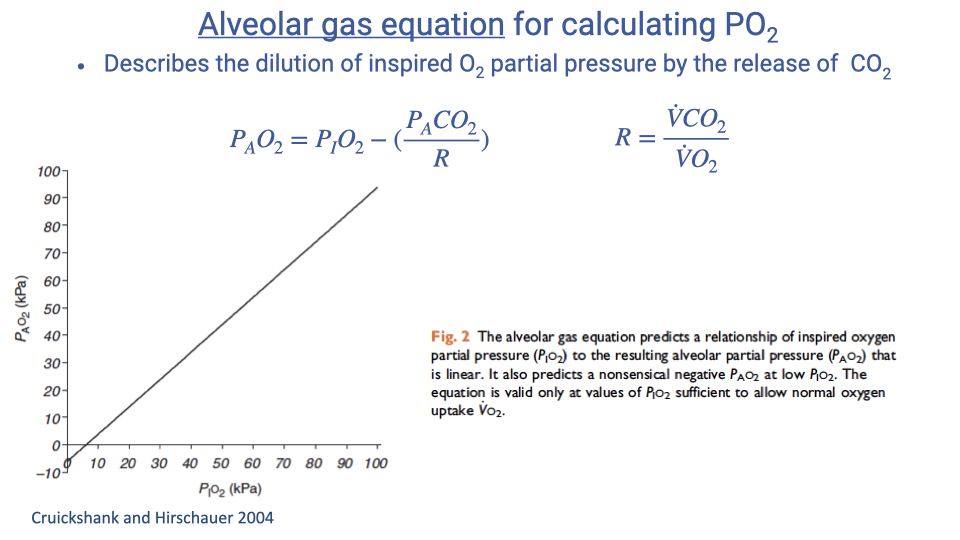
Alveolar Gas Equation for PAO2
- The alveolar gas equation calculates the partial pressure of O2 in the alveoli:
- Where $R$ is the respiratory exchange ratio (also called the respiratory quotient):
- This equation accounts for the fact that CO2 released into the alveoli dilutes the O2 present there.
- PACO2 is obtained from the clinical alveolar ventilation equation (Slide 25).
- R typically ranges from 0.7 to 1.0 depending on the metabolic substrate:
- R $\approx$ 0.7 for fat metabolism
- R $\approx$ 1.0 for carbohydrate metabolism
- R $\approx$ 0.8 is commonly assumed when the actual value is unknown.
- The graph shows a nearly linear relationship between inspired PO2 and alveolar PO2, with alveolar values always somewhat lower due to CO2 dilution and O2 uptake.
Slide 28
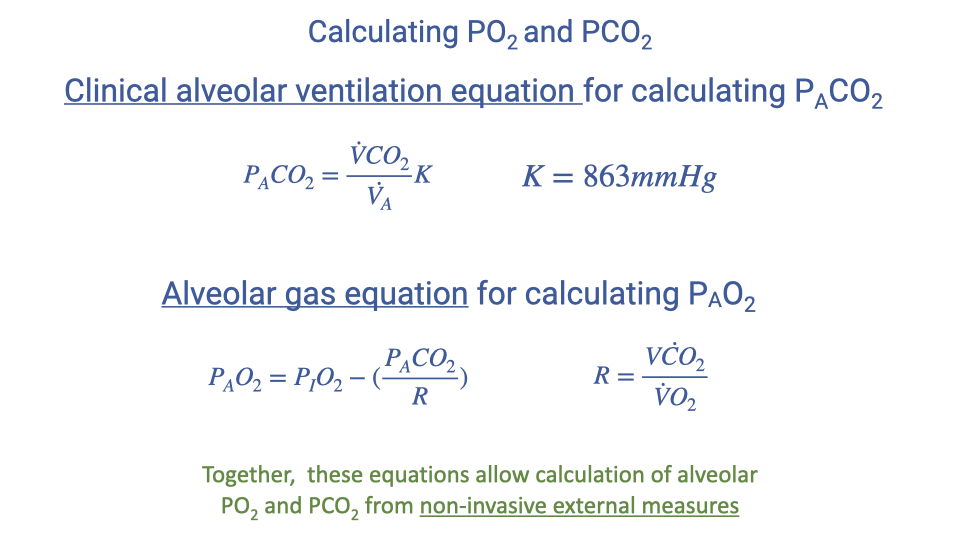
Combined Equations for Calculating Alveolar Gas Partial Pressures
- The two clinical equations work together to determine alveolar gas composition from external measurements:
Clinical alveolar ventilation equation (for PACO2):
\[P_ACO_2 = \frac{\dot{V}CO_2}{\dot{V}_A} \times K \qquad K = 863 \text{ mmHg}\]Alveolar gas equation (for PAO2):
\[P_AO_2 = P_IO_2 - \frac{P_ACO_2}{R} \qquad R = \frac{\dot{V}CO_2}{\dot{V}O_2}\]- Together, these allow calculation of alveolar PO2 and PCO2 from non-invasive external measures (spirometry-based gas analysis).
- This is clinically important because direct measurement of alveolar gas concentrations is impractical, but these values are needed to assess pulmonary function and gas exchange efficiency.
Slide 29
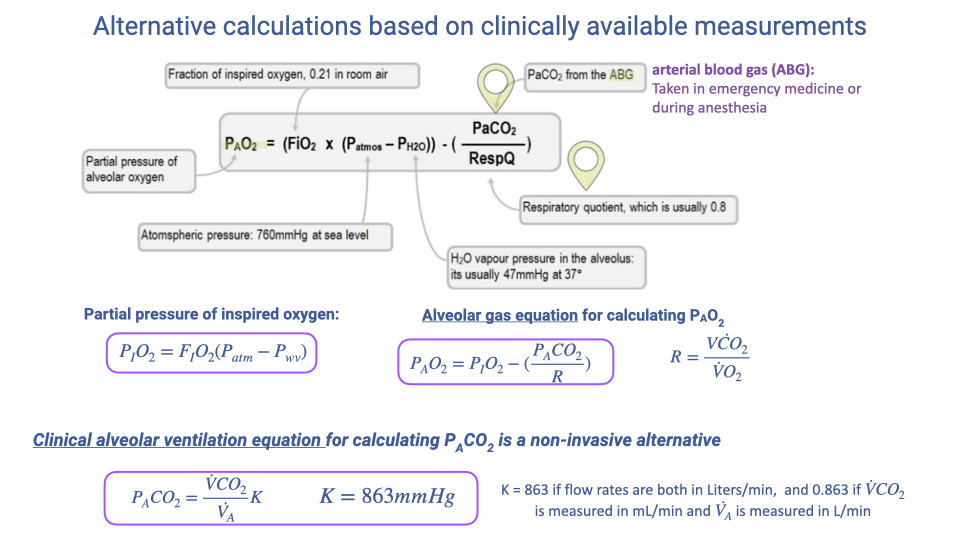
Alternative Clinical Calculations
- In clinical practice, several readily available measurements feed into these equations:
- Fraction of inspired O2 (FIO2 = 0.21 at sea level) and barometric pressure (760 mmHg at sea level) give the partial pressure of inspired O2.
- Arterial blood gas (ABG) sampling can directly provide PaCO2, which approximates PACO2.
- Pulse oximetry provides O2 saturation (SpO2), a non-invasive measure.
- The clinical alveolar ventilation equation is a non-invasive alternative for estimating PACO2 when arterial blood gas data are unavailable.
- The alveolar gas equation then uses PACO2 to estimate PAO2.
- These tools allow clinicians to assess ventilatory function in two different ways, depending on the measurements available.
Slide 30
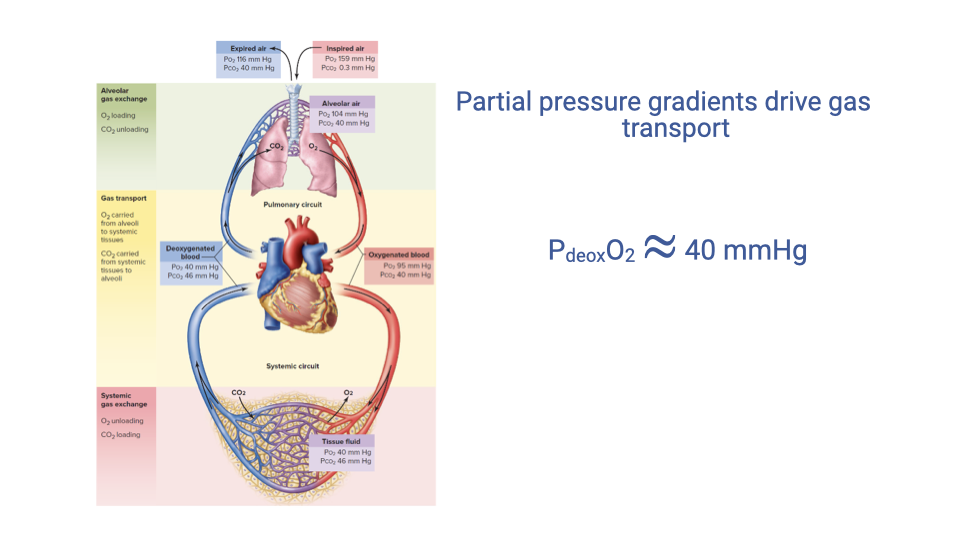
Partial Pressure Gradient for Gas Transport
- The partial pressure gradient between the alveoli and the pulmonary capillary blood is the driving force for O2 diffusion.
- At rest, the alveolar-to-capillary PO2 gradient is approximately ~60-64 mmHg (PAO2 ~100 mmHg minus PvO2 ~40 mmHg in mixed venous blood).
- The value PdeoxO2 $\approx$ 40 mmHg shown represents the approximate mixed venous (deoxygenated) PO2 entering the pulmonary capillary bed – the “starting point” for oxygenation.
- All the equations developed in this lecture – for ventilatory convection, diffusion, and alveolar gas composition – determine the magnitude of this gradient and therefore the rate of O2 transfer into the blood.
Slide 31
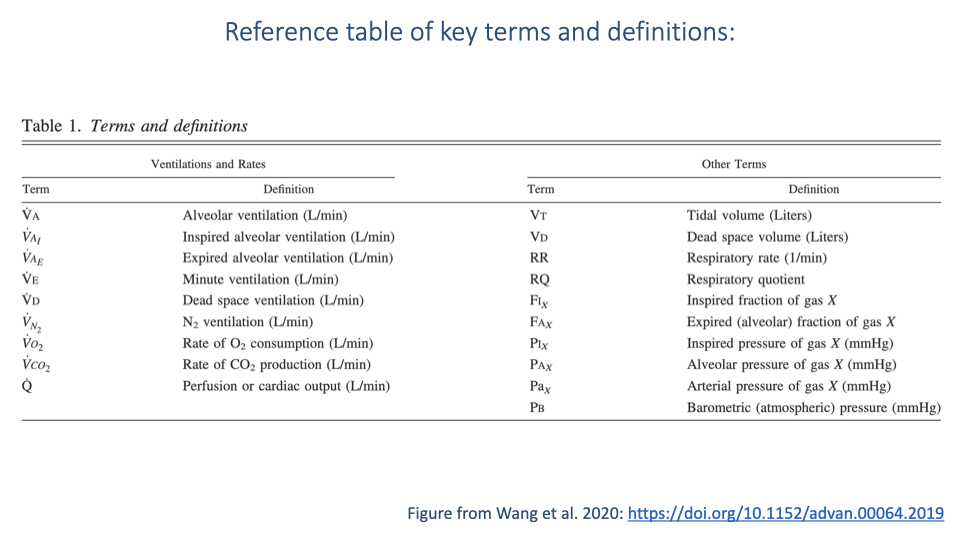
Reference Table of Key Terms and Definitions
- A comprehensive reference table of abbreviations and variables used in pulmonary gas exchange, organized into ventilation/rate terms and other terms. Adapted from Wang et al. 2020.
Ventilations and Rates
| Symbol | Definition |
|---|---|
| $\dot{V}_A$ | Alveolar ventilation (L/min) |
| $\dot{V}_I$ | Inspired alveolar ventilation (L/min) |
| $\dot{V}_E$ | Expired alveolar ventilation (L/min) |
| $\dot{V}_E$ | Minute ventilation (L/min) |
| $\dot{V}_D$ | Dead space ventilation (L/min) |
| $\dot{V}_{N_2}$ | N2 ventilation (L/min) |
| $\dot{V}O_2$ | Rate of O2 consumption (L/min) |
| $\dot{V}CO_2$ | Rate of CO2 production (L/min) |
| $\dot{Q}$ | Perfusion or cardiac output (L/min) |
Other Terms
| Symbol | Definition |
|---|---|
| $V_T$ | Tidal volume (L) |
| $V_D$ | Dead space volume (L) |
| $RR$ | Respiratory rate (breaths/min) |
| $RQ$ | Respiratory quotient |
| $F_IX$ | Inspired fraction of gas X |
| $F_AX$ | Expired (alveolar) fraction of gas X |
| $P_IX$ | Inspired pressure of gas X (mmHg) |
| $P_AX$ | Alveolar pressure of gas X (mmHg) |
| $P_aX$ | Arterial pressure of gas X (mmHg) |
| $P_B$ | Barometric (atmospheric) pressure (mmHg) |
- Reference: Wang et al. 2020, https://doi.org/10.1152/advan.00064.2019
Slide 32
Lecture 4 – Key Takeaways
- Alveolar ventilation ($\dot{V}_A = f_b \times (V_T - V_D)$) is the physiologically relevant measure of ventilation, accounting for dead space that does not contribute to gas exchange.
- The Fick principle (conservation of mass) enables calculation of $\dot{V}$O2 from externally measurable expired gas concentrations and flow rates: $\dot{V}O_2 = \dot{V}_E \times (F_IO_2 - F_EO_2)$. This is the basis for all modern metabolic testing.
- Fick’s law of diffusion governs O2 transfer across the blood-gas barrier: $\dot{V}O_2 = D_LO_2 \times \Delta P_{O_2}$. Diffusion capacity depends on surface area, membrane thickness, and the gas-specific diffusion coefficient.
- CO2 diffuses ~20 times faster than O2, so O2 diffusion is typically the rate-limiting step in pulmonary gas exchange.
- Factors that can impair pulmonary diffusion include: decreased lung surface area (fibrosis, emphysema), increased membrane thickness (inflammation, edema, fluid buildup), reduced perfusion, loss of surfactant, and reduced inspired PO2 (altitude).
- The clinical alveolar ventilation equation and the alveolar gas equation together allow estimation of alveolar PCO2 and PO2 from non-invasive measurements.
Slide 33
Practice Problem: Alveolar PO2 on 100% O2
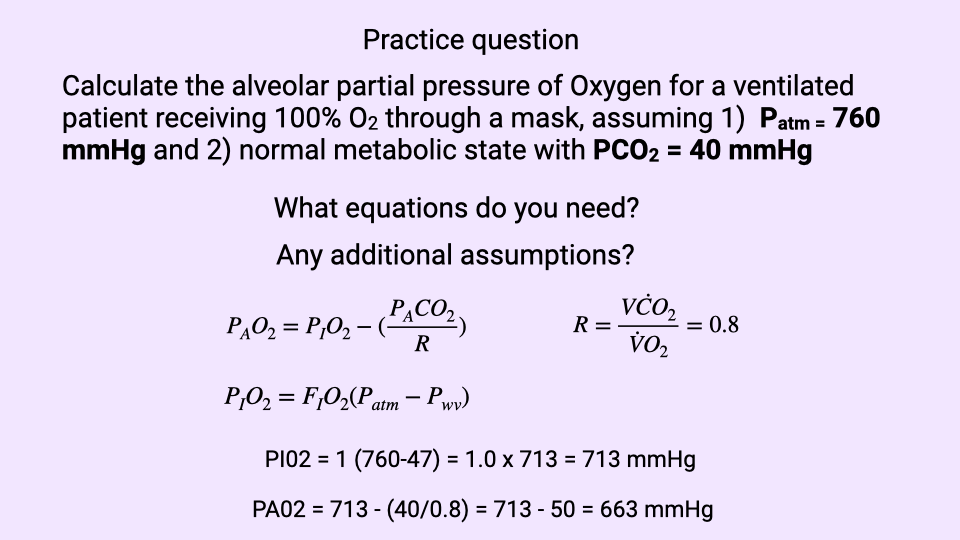
Problem. Calculate the alveolar partial pressure of oxygen ($P_AO_2$) for a ventilated patient receiving 100% O2 through a mask, given:
- $P_{atm} = 760$ mmHg
- Normal metabolic state with $P_ACO_2 = 40$ mmHg
What equations are needed?
The alveolar gas equation, combined with the equation for the inspired partial pressure of O2 (corrected for water vapor in the conducting airways):
\[P_AO_2 = P_IO_2 - \frac{P_ACO_2}{R}\] \[P_IO_2 = F_IO_2 \times (P_B - P_{H_2O})\]Additional assumptions.
- $F_IO_2 = 1.0$ (100% O2 delivered by the mask)
- $P_{H_2O} = 47$ mmHg (saturated water vapor pressure at body temperature, 37 °C)
- $R \approx 0.8$ (typical respiratory exchange ratio for mixed substrate metabolism)
Step 1 – Calculate $P_IO_2$:
\[P_IO_2 = 1.0 \times (760 - 47) = 713 \text{ mmHg}\]Step 2 – Calculate $P_AO_2$:
\[P_AO_2 = 713 - \frac{40}{0.8} = 713 - 50 = 663 \text{ mmHg}\]Result. The alveolar PO2 for a patient breathing 100% O2 is approximately 663 mmHg – roughly 6-fold higher than the typical ~100 mmHg on room air. This illustrates how supplemental O2 dramatically increases the alveolar-to-capillary PO2 gradient, which is the driving force for O2 diffusion across the blood-gas barrier and a primary therapeutic strategy for patients with impaired pulmonary gas exchange.
Key Equations
| Equation | Name | Description |
|---|---|---|
| $\dot{V}_A = f_b \times (V_T - V_D)$ | Alveolar ventilation rate | Rate of air reaching gas exchange surfaces, accounting for dead space |
| $V_{D,\text{phys}} = V_{D,\text{alveolar}} + V_{D,\text{anatomic}}$ | Physiological dead space | Total dead space is the sum of anatomical and alveolar components |
| $\dot{V}_E = f_b \times V_T$ | Minute ventilation | Total rate of air movement in and out of the lungs per minute |
| $M_x = M_{x,\text{in}} - M_{x,\text{out}}$ | Fick principle | Conservation of mass: uptake equals difference between input and output |
| $\dot{V}O_2 = \dot{V}_E \times (F_IO_2 - F_EO_2)$ | Fick principle for O2 | O2 consumption from expired ventilation and gas fractions |
| $\dot{V}O_2 = \frac{A \times D \times \Delta P_{O_2}}{T}$ | Fick’s law of diffusion | Diffusion rate depends on area, coefficient, gradient, and thickness |
| $D_LO_2 = \frac{A \times D}{T}$ | Diffusion capacity of the lungs | Combined structural factors determining lung diffusion capacity |
| $\dot{V}O_2 = D_LO_2 \times \Delta P_{O_2}$ | Simplified diffusion equation | O2 transfer rate equals diffusion capacity times pressure gradient |
| $P_ACO_2 = \frac{\dot{V}CO_2}{\dot{V}_A} \times K$ | Clinical alveolar ventilation equation | Estimates alveolar PCO2 from CO2 output and alveolar ventilation; $K = 863$ mmHg |
| $P_AO_2 = P_IO_2 - \frac{P_ACO_2}{R}$ | Alveolar gas equation | Estimates alveolar PO2 accounting for CO2 dilution |
| $R = \frac{\dot{V}CO_2}{\dot{V}O_2}$ | Respiratory exchange ratio | Ratio of CO2 production to O2 consumption; typically 0.7–1.0 |
Glossary of Key Terms
| Term | Definition |
|---|---|
| Alveolar ventilation ($\dot{V}_A$) | The volume of air per minute that reaches the alveolar gas exchange surfaces; equals breathing frequency times (tidal volume minus dead space volume). |
| Minute ventilation ($\dot{V}_E$) | The total volume of air moved in and out of the lungs per minute; also called expired minute ventilation. |
| Anatomical dead space | The volume of conducting airways (trachea, bronchi, bronchioles) that do not participate in gas exchange; approximately 150 mL in healthy adults. |
| Alveolar dead space | The volume of alveoli that are ventilated but not perfused with capillary blood, and therefore do not contribute to gas exchange. |
| Physiological dead space | The total non-functional ventilatory volume: anatomical dead space plus alveolar dead space. In healthy individuals, approximately equal to anatomical dead space. |
| Fick principle | A method based on the law of conservation of mass used to calculate the rate of gas uptake or release by measuring the difference between input and output concentrations. |
| Fick’s law of diffusion | A physical law stating that the rate of diffusion of a gas across a tissue barrier is proportional to the surface area and partial pressure gradient, and inversely proportional to the barrier thickness. |
| Diffusion capacity of the lungs (DLO2) | A composite measure combining lung surface area, membrane thickness, and the gas-specific diffusion coefficient; determines the structural capacity for gas transfer. |
| Blood-gas barrier | The thin tissue separating alveolar air from capillary blood, consisting of alveolar epithelium, fused basement membranes, and capillary endothelium (~0.5 micrometers thick). |
| Partial pressure gradient ($\Delta P_{O_2}$) | The difference in partial pressure of O2 between the alveolus and the capillary blood; the driving force for O2 diffusion into the blood. |
| Diffusion coefficient (D) | A constant specific to each gas that describes its rate of diffusion through a given medium. CO2 has a diffusion coefficient approximately 20 times greater than O2. |
| $\dot{V}$O2 max | The maximum rate of oxygen consumption during intense exercise; a key measure of aerobic capacity and athletic performance. |
| Hyperventilation | Breathing at a rate that exceeds metabolic demand, causing excessive CO2 loss, respiratory alkalosis, and potentially loss of consciousness. |
| Hypoventilation | Breathing at a rate insufficient for metabolic demand, leading to CO2 accumulation, reduced alveolar O2, and respiratory acidosis. Often seen with drug-induced respiratory depression or obstructive lung diseases. |
| Respiratory exchange ratio (R) | The ratio of CO2 production to O2 consumption ($\dot{V}$CO2 / $\dot{V}$O2); typically ranges from 0.7 (fat metabolism) to 1.0 (carbohydrate metabolism), with 0.8 used as a default estimate. |
| Clinical alveolar ventilation equation | An equation that estimates alveolar PCO2 from the ratio of CO2 production to alveolar ventilation, using a constant K = 863 mmHg. |
| Alveolar gas equation | An equation that estimates alveolar PO2 from inspired PO2 and alveolar PCO2, accounting for the dilution effect of CO2 in the alveolar space. |
| Capacitance coefficient ($\beta_{gO_2}$) | A constant describing the amount of O2 that can be carried per unit volume of air per unit partial pressure difference. |
| Surfactant | A substance produced by alveolar cells that reduces surface tension, preventing alveolar collapse and maintaining surface area for gas exchange. |
| Arterial blood gas (ABG) | A clinical test that directly measures the partial pressures of O2 and CO2, as well as pH, in arterial blood. |
| Pulse oximetry (SpO2) | A non-invasive method for monitoring oxygen saturation of hemoglobin in peripheral blood. |