Lecture 3: The Oxygen Supply Cascade and Ventilation
Slide 1
- This lecture focuses on the first step of the oxygen supply cascade: pulmonary and alveolar ventilation — getting air from the environment into the lungs and to the gas exchange surfaces.
- Subsequent lectures will build up the remaining steps, introducing governing equations at each stage to understand what limits oxygen delivery during exercise.
Slide 2
Learning objectives
- Describe the steps in the oxygen supply cascade from the environment to the mitochondria.
- Describe the path of air into the lungs.
- Define dead space volume and discuss factors that contribute to it.
- Describe the factors that contribute to minute ventilation and alveolar ventilation.
Slide 3
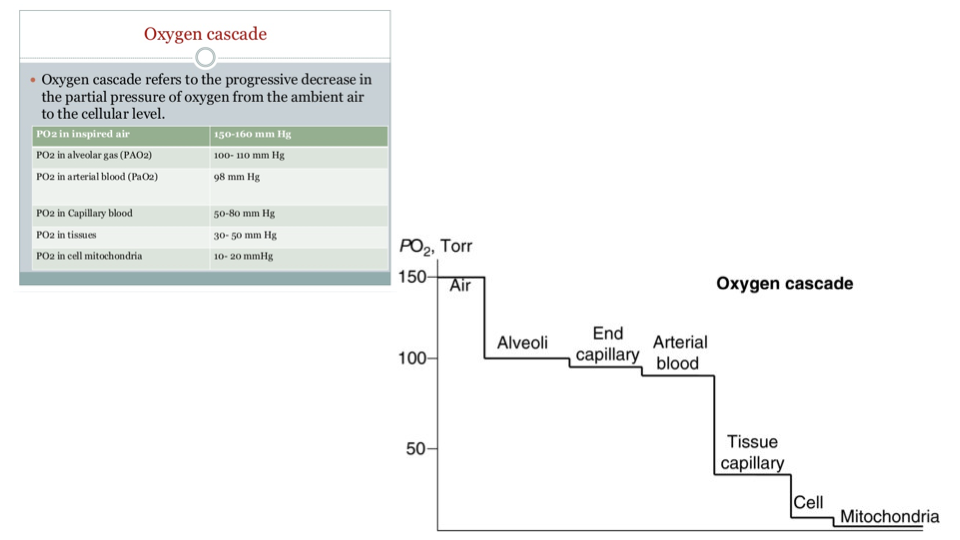
The oxygen cascade
- The oxygen cascade refers to the progressive decrease in PO₂ from ambient air (~150 mmHg) to the cellular mitochondria (~10–20 mmHg).
- PO₂ drops at each step because oxygen is consumed or diluted as it moves through the system.
| Location | PO₂ (mmHg) |
|---|---|
| Inspired air | ~150 |
| Alveolar gas | 100–110 |
| Arterial blood | ~98 |
| Capillary blood | 30–60 |
| Tissues | 20–30 |
| Cell mitochondria | 10–20 |
- By learning the equations governing each step, the physical factors limiting oxygen supply can be identified under different conditions (e.g., normoxia, hypoxia, diving).
Slide 4
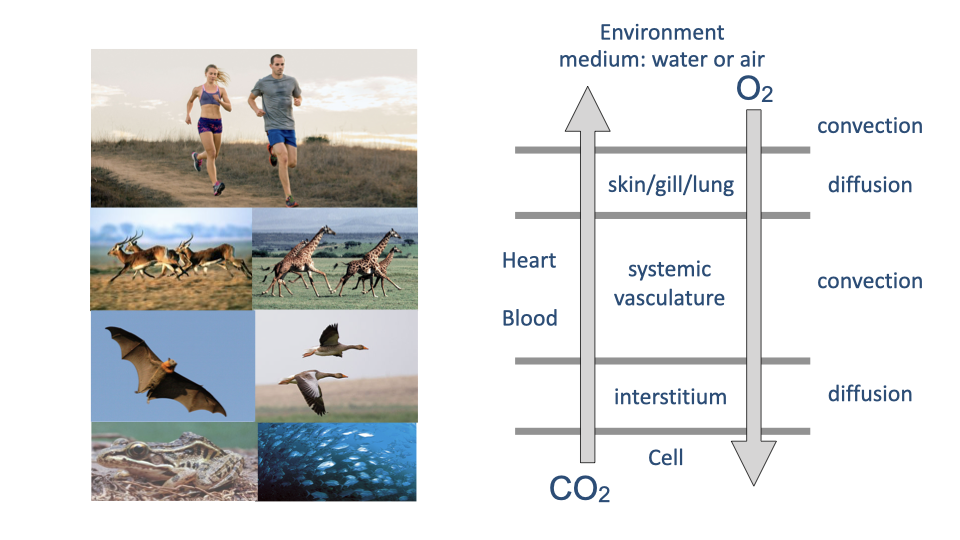
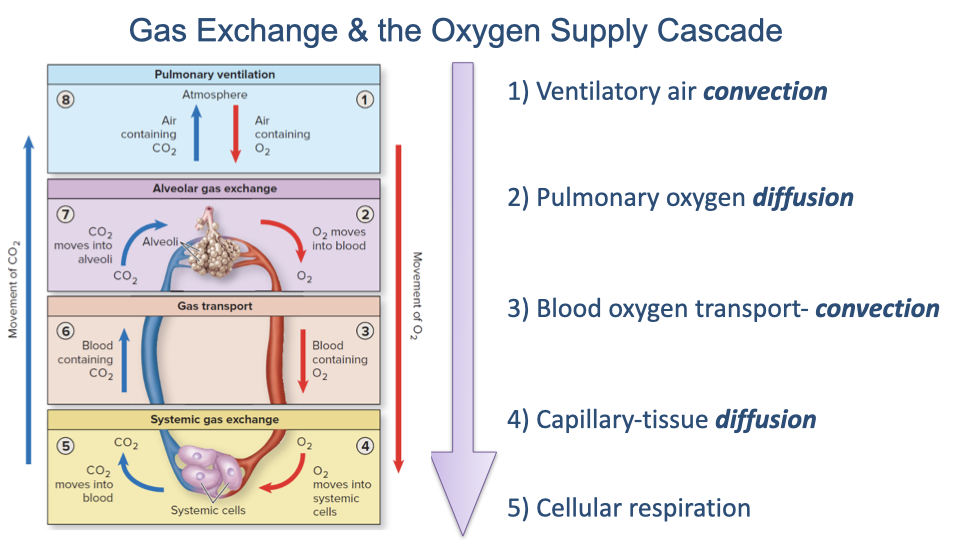
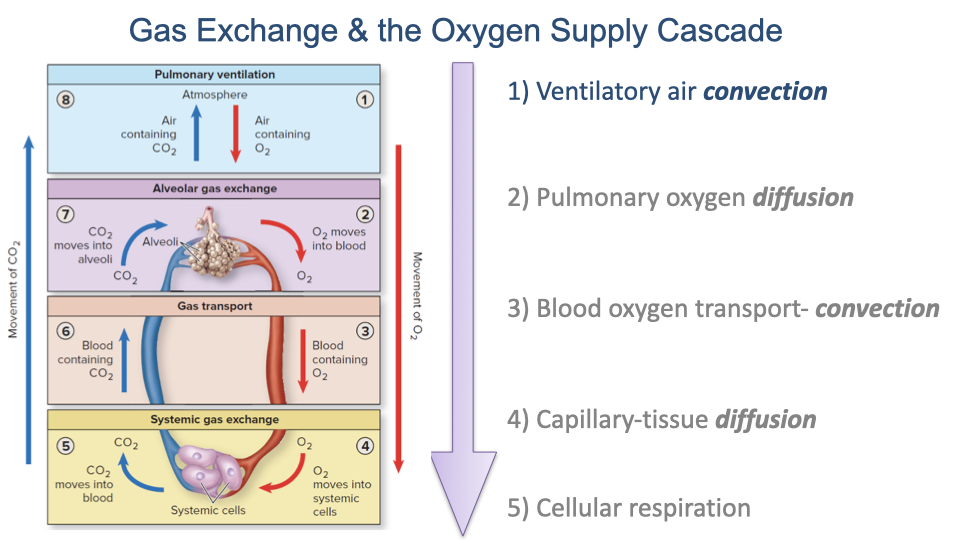
- Gas exchange follows a series of alternating convection and diffusion steps.
- Convection (bulk flow) moves gases over long distances — ventilation moves air into the lungs; the circulatory system transports oxygen in blood.
- Diffusion moves gases across thin barriers — at the lung surface and at the tissue capillaries.
- CO2 flows in the reverse direction, from cells to the environment.
- The fundamental principles are shared across vertebrates, though the structures differ (gills, lungs, parabronchial systems).
Slide 5
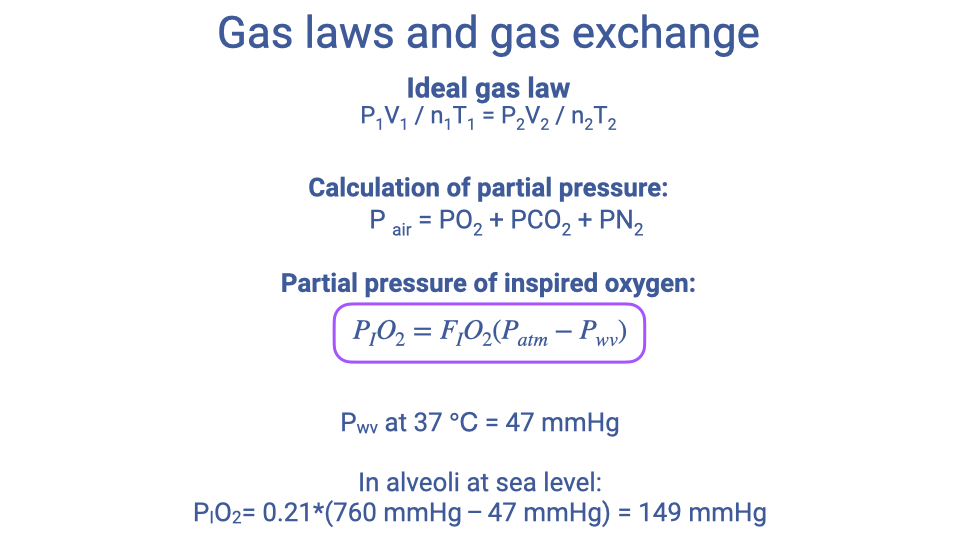
Review: Gas laws applied to ventilation
- The ideal gas law and Dalton’s law (from Lecture 2) provide the foundation for calculating oxygen availability.
- The key equation for the top of the oxygen cascade is:
- At sea level and body temperature (37°C):
- FIO2 = 0.21 (fractional concentration of O2 in air) is approximately constant and used for all calculations in this course.
- PH₂O = 47 mmHg at body temperature, and must be subtracted because water vapor dilutes the inspired air.
- This value (149 mmHg) represents PO₂ at the top of the cascade — it does not indicate how much oxygen actually reaches the gas exchange surfaces.
Slide 6
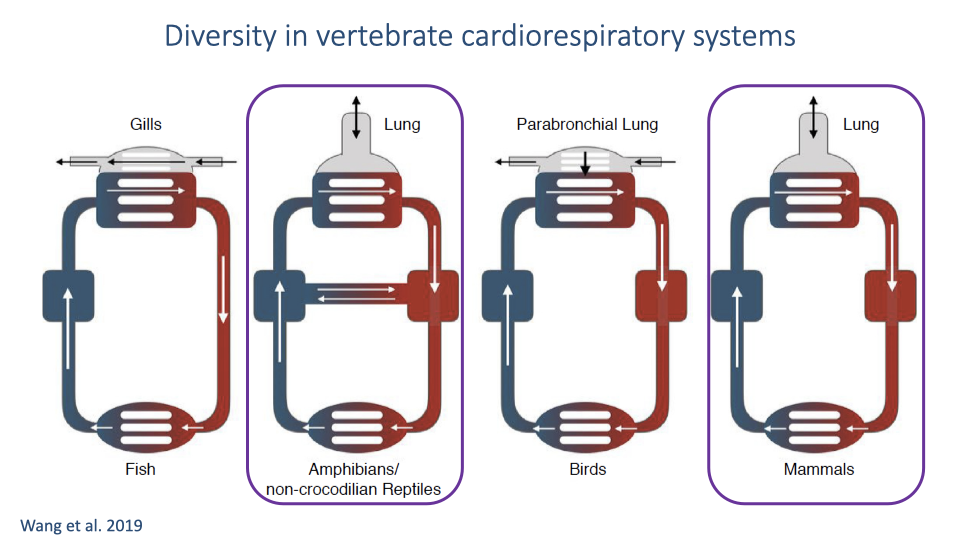
Diversity of gas exchange structures
- Fish — Water flows over gills in a countercurrent exchange system (water and blood flow in opposite directions), maximizing O2 extraction.
- Birds — Air flows through parabronchial lungs in a cross-current pattern (air flow perpendicular to blood flow). This is highly efficient and contributes to birds’ success at high altitudes.
- Amphibians, non-crocodilian reptiles, and mammals — Use tidally ventilated lungs where air flows in and out through the same passages. Air reverses direction, creating a “pool” exchange system. This is the ancestral condition for tetrapods.
- Key difference: In gills and parabronchial lungs, there is no anatomical dead space because airflow is unidirectional. In tidally ventilated lungs, air cannot be fully emptied with each breath, resulting in anatomical dead space that dilutes the oxygen reaching the gas exchange surfaces.
Slide 7
Step 1: Ventilatory air convection
- The oxygen supply cascade is built up step by step, with governing equations introduced at each stage.
- This lecture focuses on Step 1: ventilatory air convection — the tidal ventilation of the lungs.
- Topics include lung structure and function, the mechanics of breathing, dead space, and the distinction between pulmonary and alveolar ventilation.
- Understanding the factors that limit lung performance provides the foundation for discussing exercise limitations and hypoxia in later lectures.
Slide 8
- This section covers the functional organization of the mammalian respiratory system, focusing on features important for oxygen delivery rather than detailed anatomical memorization.
Slide 9
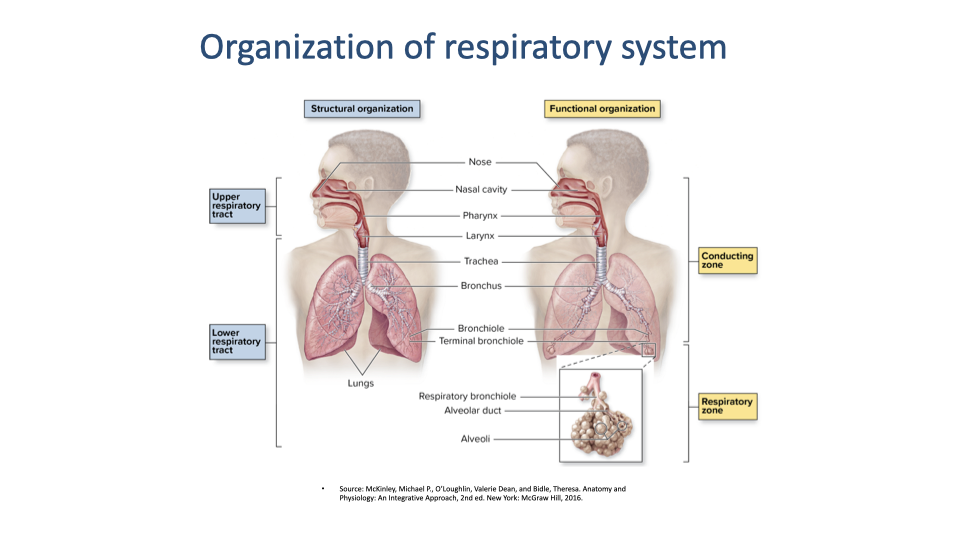
- The respiratory system includes the upper airway (nasal cavity, pharynx, larynx) and the lower airway (trachea, bronchi, bronchioles, alveoli).
- The focus is on functional organization rather than memorization of anatomical detail — understanding which structures participate in gas exchange and which do not.
- The respiratory system is divided into two functional zones: the conducting zone (upper airway, trachea, and bronchi), which transports air but does not participate in gas exchange, and the respiratory zone, containing the smallest respiratory bronchioles and alveoli, where gas exchange occurs. The branching of airways into many small alveolar spaces provides a large surface area for respiratory gas exchange.
Slide 10
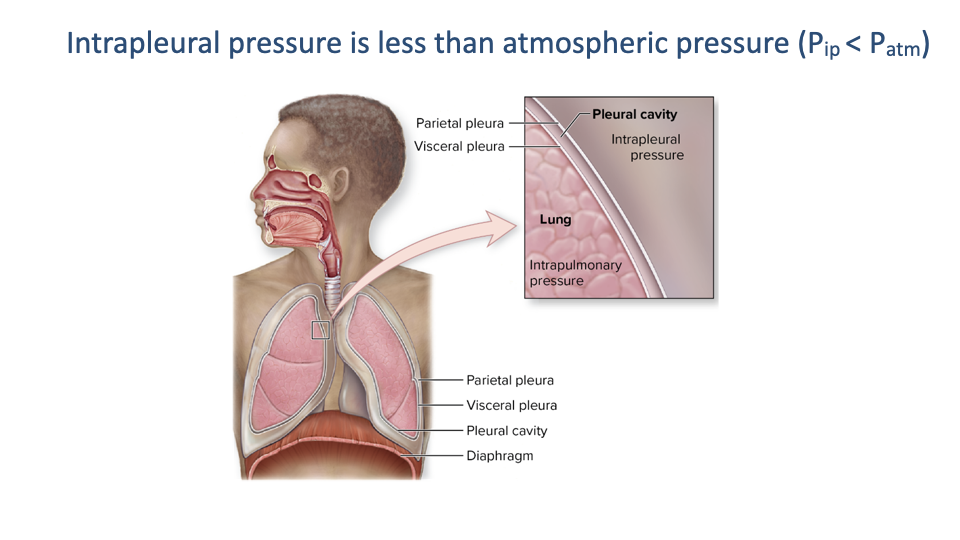
Intrapleural pressure
- The lungs are surrounded by a thin pleural cavity between the visceral pleura (on the lung surface) and the parietal pleura (on the chest wall).
- Intrapleural pressure is negative (below atmospheric pressure), which keeps the lungs inflated against the chest wall.
- Ventilation depends on managing changes in air pressure and airway resistance to move air in and out of the lungs.
Slide 11
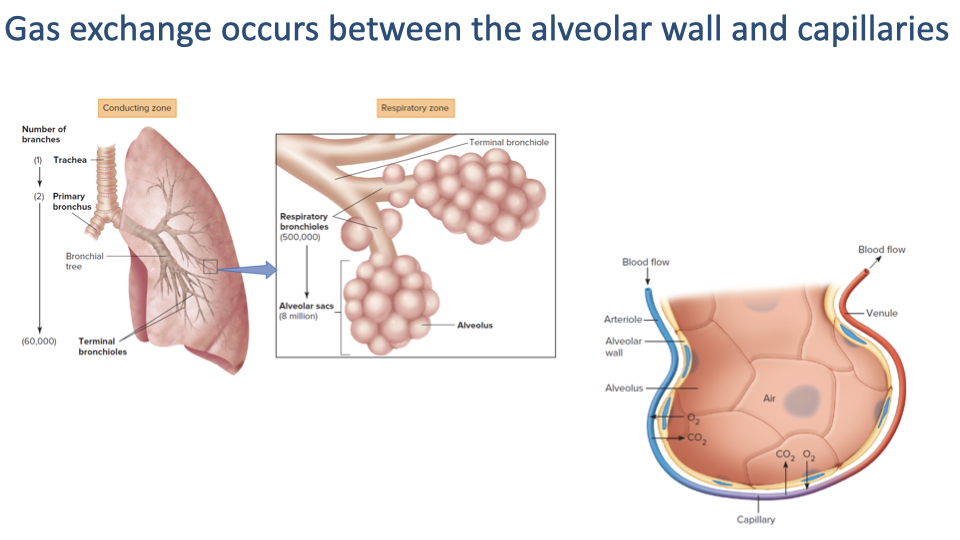
The blood-gas barrier
- Gas exchange occurs at the alveoli, where the alveolar wall is in close contact with pulmonary capillaries.
- For effective gas exchange, three conditions must be met:
- Air must reach the alveolar space.
- Deoxygenated blood must flow through the capillaries surrounding the alveoli.
- The barrier between the alveolar surface and capillary blood must be thin enough to allow efficient diffusion.
Slide 12
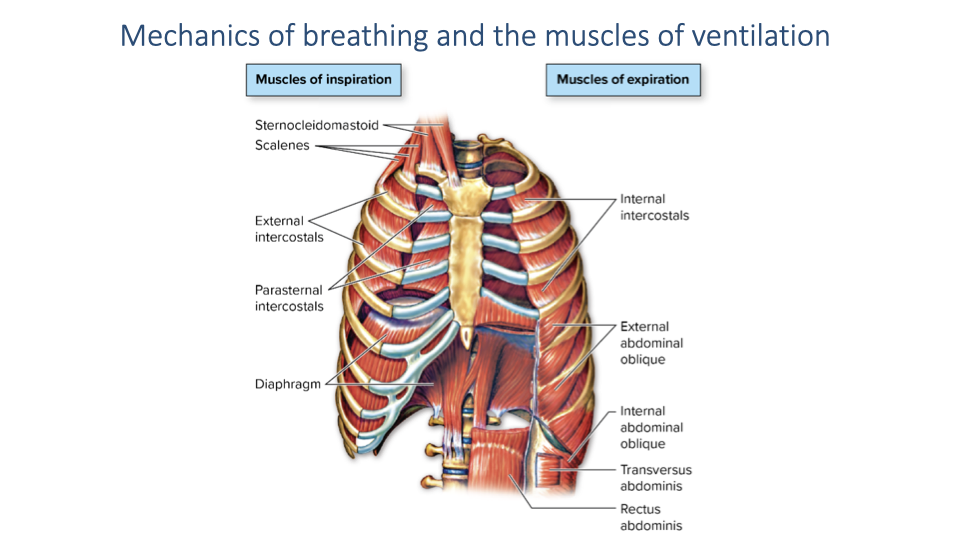
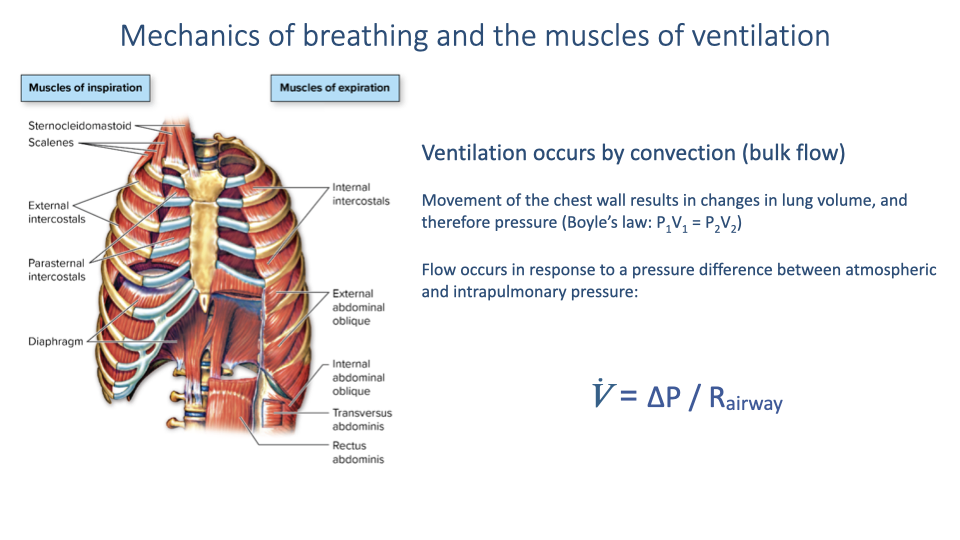
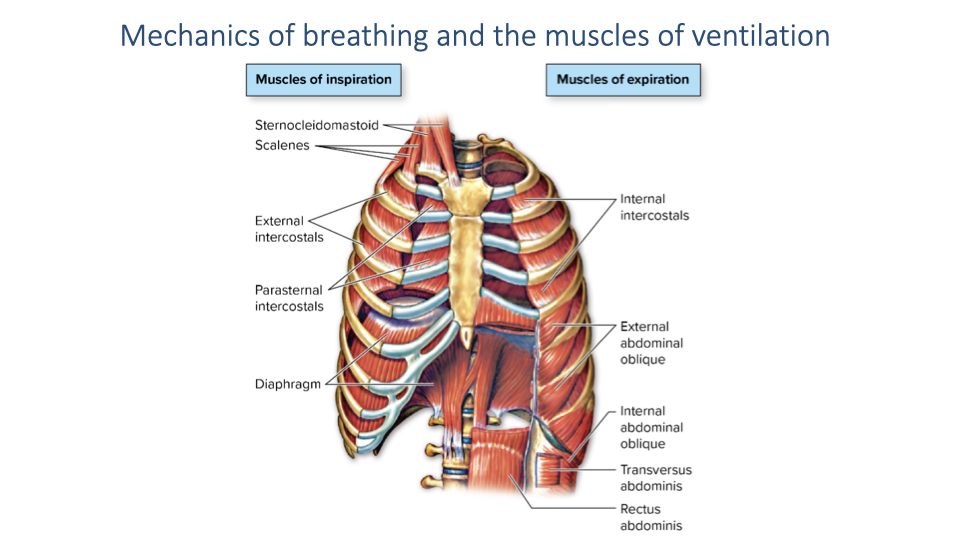
Muscles of ventilation
Muscles of inspiration:
- Diaphragm — the primary muscle of inspiration in mammals
- External intercostals and parasternal intercostals — assist in expanding the rib cage
- Accessory muscles (sternocleidomastoid, scalenes) — recruited during forced breathing or exercise; largely inactive during quiet breathing
Muscles of expiration:
- Internal intercostals — active during forced exhalation
- Abdominal muscles (external oblique, internal oblique, transversus abdominis, rectus abdominis) — contract to increase abdominal pressure and push the diaphragm upward during forced exhalation
- During quiet breathing, exhalation is largely passive, driven by the elastic recoil of the lungs and rib cage.
Slide 13
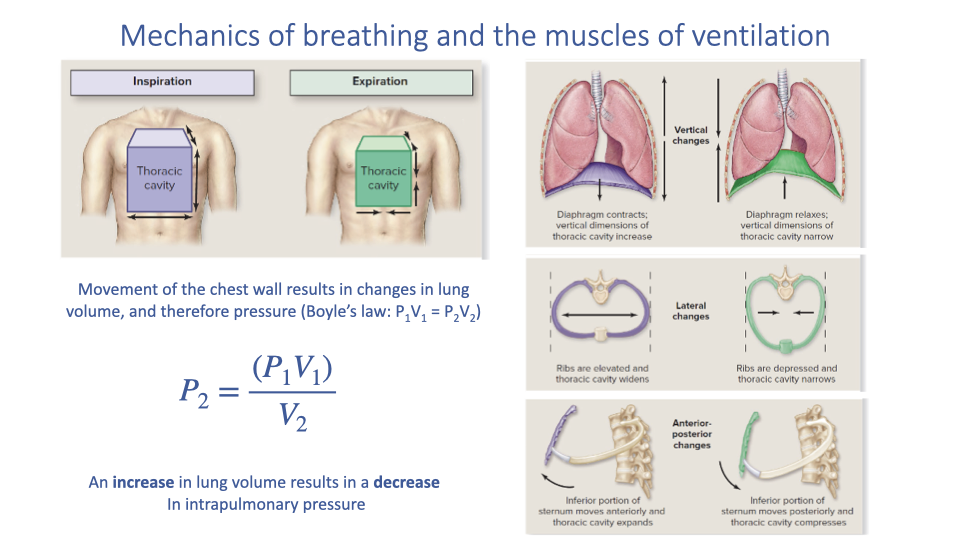
Breathing mechanics and Boyle’s Law
- The diaphragm has a complex 3D dome shape. When it contracts, it flattens, increasing thoracic volume by:
- Moving downward (increasing vertical space)
- Pushing the lower ribs outward (increasing lateral space)
- Pushing the sternum forward (increasing anterior-posterior space)
- Boyle’s Law governs the resulting pressure change:
- An increase in lung volume during inspiration causes a decrease in intrapulmonary pressure, drawing air into the lungs.
- During expiration, the volume decreases, pressure rises, and air flows out.
Slide 14
Airflow equation
- Ventilation occurs by convection (bulk flow) driven by pressure differences.
- The rate of airflow is determined by:
- Where $\dot{V}$ is the volume flow rate, $\Delta P$ is the pressure difference between intrapulmonary and atmospheric pressure, and $R_{airway}$ is the resistance of the airways.
- Two factors govern airflow:
- The pressure difference generated by thoracic volume changes
- The airway resistance, which depends on airway diameter
Slide 15
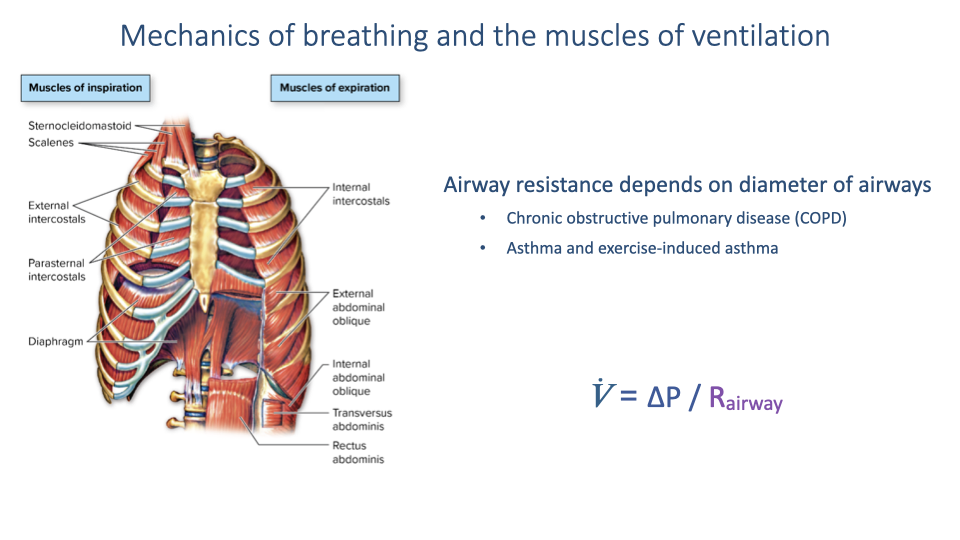
Airway resistance — Clinical relevance
- Airway resistance is clinically important because it can vary substantially in disease:
- Chronic Obstructive Pulmonary Disease (COPD) — fibrosis and scarring reduce airway elasticity and increase resistance.
- Asthma (including exercise-induced asthma) — acute inflammation narrows airways, increasing resistance.
- When airway resistance increases, a greater pressure difference is required to maintain the same flow rate, significantly increasing the muscular work of breathing.
Slide 16
Breathing exercise — Exploring ventilation mechanics
Four breathing exercises highlight differences in muscle recruitment:
- Quiet breathing — Primarily diaphragmatic; exhalation is nearly passive (elastic recoil). People often do not notice intercostal involvement during quiet breathing, though it varies with habitual patterns and stress levels.
- Maximum inspiration + forced exhalation — Recruits intercostals, abdominal muscles, and accessory muscles (sternocleidomastoid, scalenes, trapezius, pectoralis).
- Maximum inspiration + slow exhalation — Involves controlled resistance to lung recoil; individuals may purse their lips to increase airway resistance and slow the flow rate (applying $\dot{V} = \Delta P / R$).
- Belly breathing — Focuses on diaphragm-driven breathing with minimal rib cage movement. Used as a meditative practice to reduce anxiety, because chronic stress often causes habitual recruitment of accessory muscles even during quiet breathing, increasing the perceived effort of breathing.
Slide 17
- This slide serves as a reference during the breathing exercise discussion.
- Inspiration muscles are listed on the left; expiration muscles on the right.
- In practice, the division is not absolute — the intercostals contribute to both phases at different times.
Slide 18
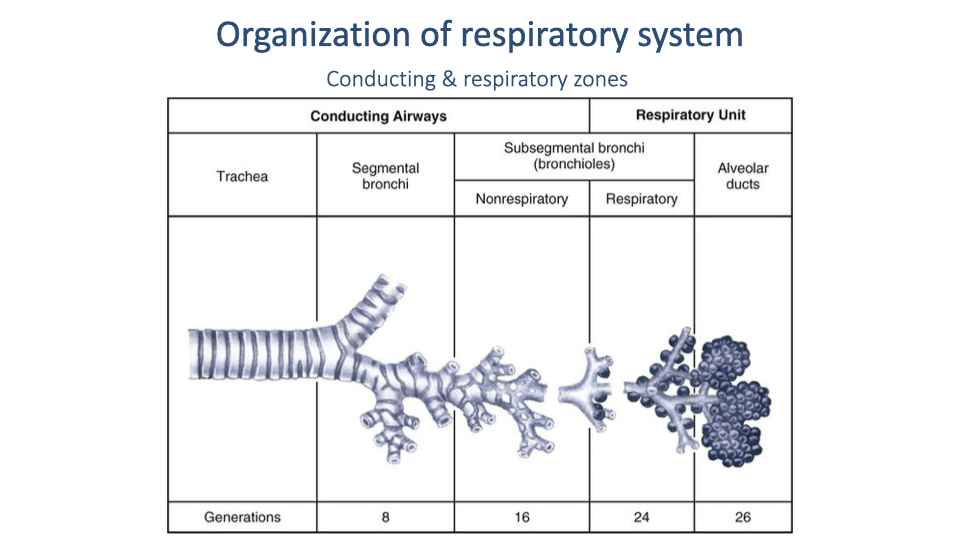
Conducting zone vs. respiratory zone
- The airways are divided into two functional regions:
- Conducting zone (generations 0–16): Trachea, bronchi, and bronchioles that transport air but do not participate in gas exchange. This constitutes the anatomical dead space.
- Respiratory zone (generations 17–23): Respiratory bronchioles, alveolar ducts, and alveolar sacs where the tissue barrier is thin enough for gas exchange by diffusion.
- The branching pattern creates enormous increases in total cross-sectional area and surface area in the respiratory zone.
Slide 19
- Returning to the oxygen supply cascade framework: this lecture is building up the equations for Step 1 (ventilatory air convection).
- The equations introduced here will determine how much oxygen is transported to the alveolar gas exchange surfaces.
Slide 20
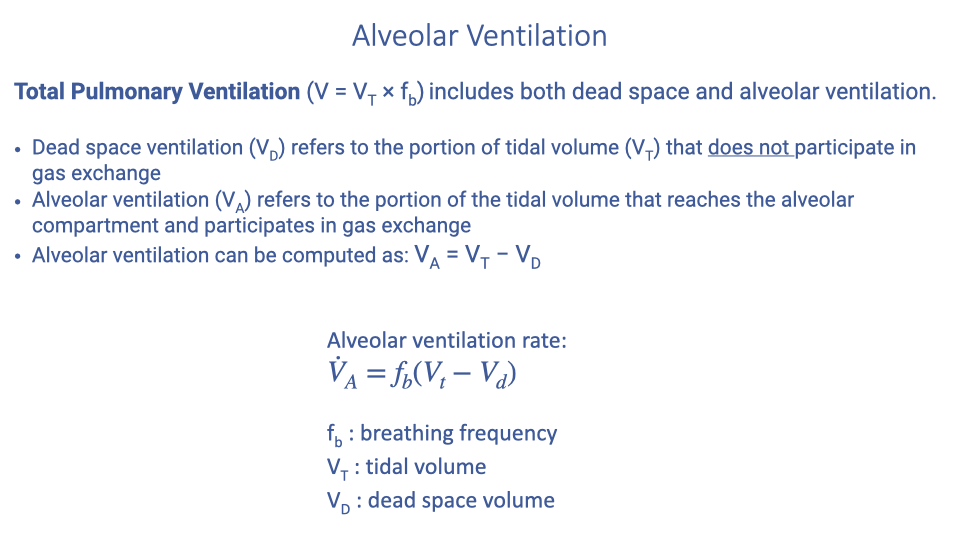
Total pulmonary ventilation and alveolar ventilation
- Total pulmonary ventilation ($\dot{V}_E$) includes both dead space and alveolar ventilation:
- Dead space ventilation ($V_D$) — the portion of tidal volume that does not participate in gas exchange (air in the conducting airways).
- Alveolar ventilation ($V_A$) — the portion that reaches the alveolar compartment and participates in gas exchange.
- The alveolar ventilation rate:
- Where $f_b$ = breathing frequency, $V_T$ = tidal volume, $V_D$ = dead space volume.
- Dead space ventilation is functionally important because it reduces the amount of oxygen reaching the gas exchange surfaces.
Slide 21
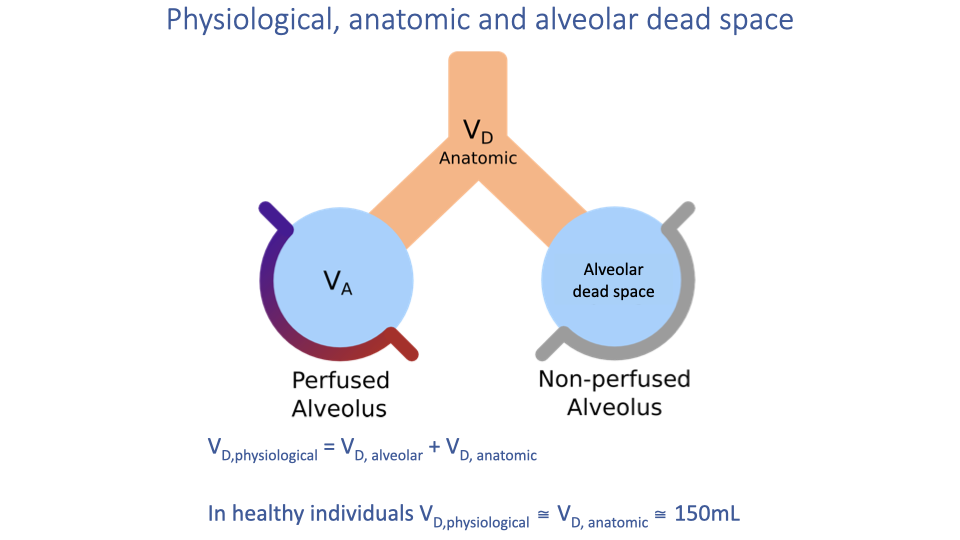
Types of dead space
- Anatomical dead space — the volume of the conducting airways (trachea, bronchi, bronchioles) that do not participate in gas exchange. Approximately 150 mL in a healthy adult.
- Alveolar dead space — alveoli that are ventilated but not perfused with blood, so no gas exchange occurs (e.g., during rest when only a subset of the pulmonary capillary bed is recruited).
- Physiological dead space = anatomical dead space + alveolar dead space:
- In healthy individuals, physiological dead space is approximately equal to anatomical dead space (~150 mL).
- During exercise, pulmonary perfusion increases and more alveoli become perfused, reducing alveolar dead space and increasing the effective gas exchange surface.
- In disease (e.g., pneumonia), fluid or scarring can prevent gas exchange in affected alveoli, increasing physiological dead space.
Slide 22
Minute ventilation vs. alveolar ventilation — Example
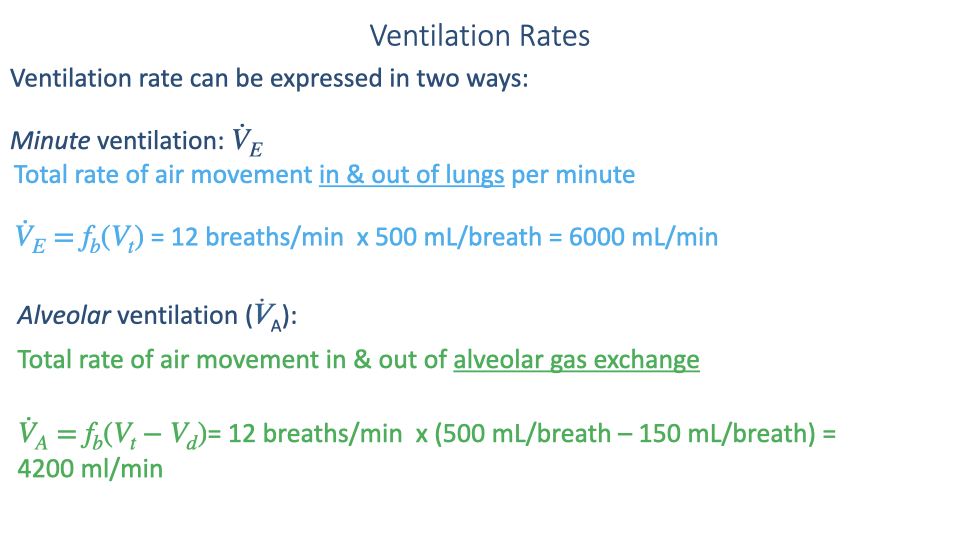
Minute (pulmonary) ventilation — total air moved in and out of the lungs per minute:
\[\dot{V}_E = f_b \times V_T = 12 \times 500 = 6000 \text{ mL/min}\]Alveolar ventilation — air reaching the gas exchange surfaces per minute:
\[\dot{V}_A = f_b \times (V_T - V_D) = 12 \times (500 - 150) = 4200 \text{ mL/min}\]- In this example, 30% of each breath (150 mL out of 500 mL) is wasted in dead space.
- The distinction is functionally important: only alveolar ventilation contributes to oxygen uptake and CO2 elimination.
Slide 23
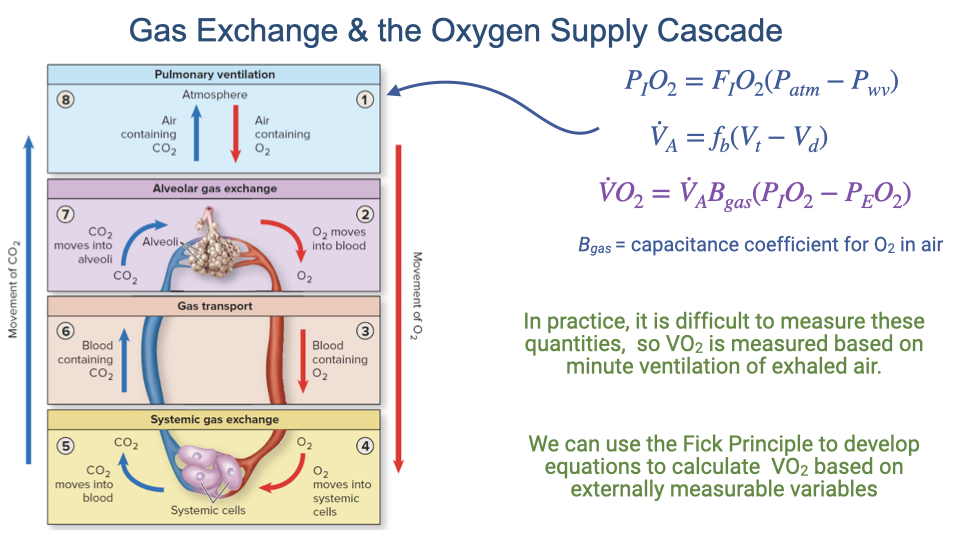
Oxygen delivery at Step 1 — Building the equation
- The partial pressure of inspired oxygen sets the starting point:
- The alveolar ventilation rate determines how much air reaches the exchange surfaces:
- The amount of oxygen actually delivered to the alveoli can be expressed as:
- Where $\beta_{gO_2}$ is the capacitance coefficient for O2 in air, and $P_EO_2$ is the partial pressure of O2 in exhaled air.
- In practice, these partial pressures are difficult to measure directly. The Fick Principle (introduced in the next lecture) provides a more practical approach to calculating $\dot{V}O_2$ from externally measurable variables.
Slide 24
Spirometry
- Spirometry is the clinical and research tool used to measure lung volumes and airflow rates.
- The patient breathes through a mouthpiece connected to a device that measures the rate and volume of exhaled air.
- Spirometry is used in:
- Clinical settings — to test lung function and diagnose obstructive or restrictive lung diseases.
- Exercise physiology labs — with a face mask to measure ventilation rates and calculate $\dot{V}O_2$ during exercise.
Slide 25
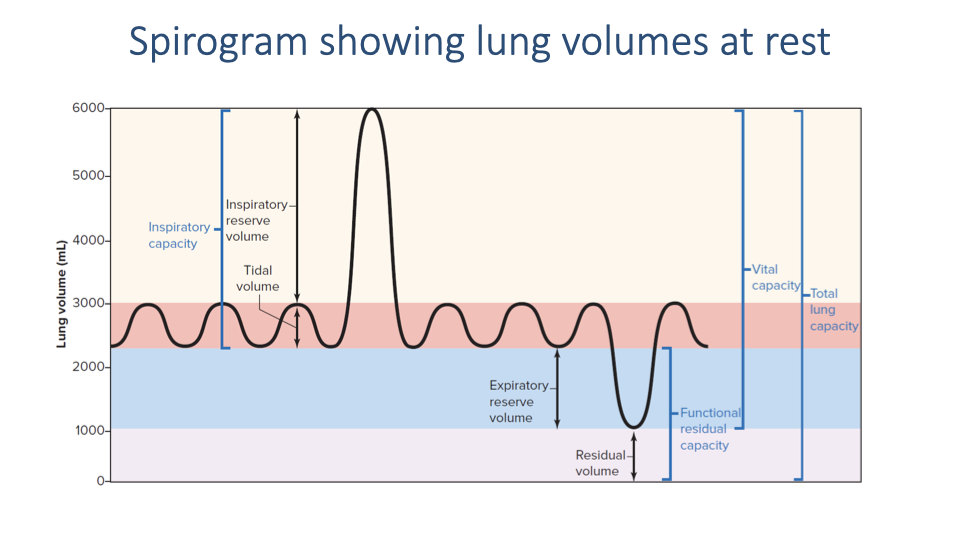
Lung volumes and capacities
| Term | Definition |
|---|---|
| Tidal volume (VT) | Volume of air inhaled or exhaled in a normal breath (~500 mL at rest) |
| Inspiratory reserve volume (IRV) | Additional volume that can be inhaled beyond a normal tidal inhalation |
| Expiratory reserve volume (ERV) | Additional volume that can be exhaled beyond a normal tidal exhalation |
| Residual volume (RV) | Air remaining in the lungs after maximum exhalation; cannot be measured by spirometry |
| Vital capacity (VC) | Total usable lung volume = IRV + VT + ERV |
| Total lung capacity (TLC) | VC + RV; the maximum volume the lungs can hold |
| Functional residual capacity (FRC) | ERV + RV; the volume remaining after a normal exhalation |
| Inspiratory capacity (IC) | VT + IRV; the maximum volume that can be inhaled from the end of a normal exhalation |
- Changes in these volumes during exercise (e.g., increased tidal volume, decreased reserve volumes) are examined in later lectures.
Slide 26
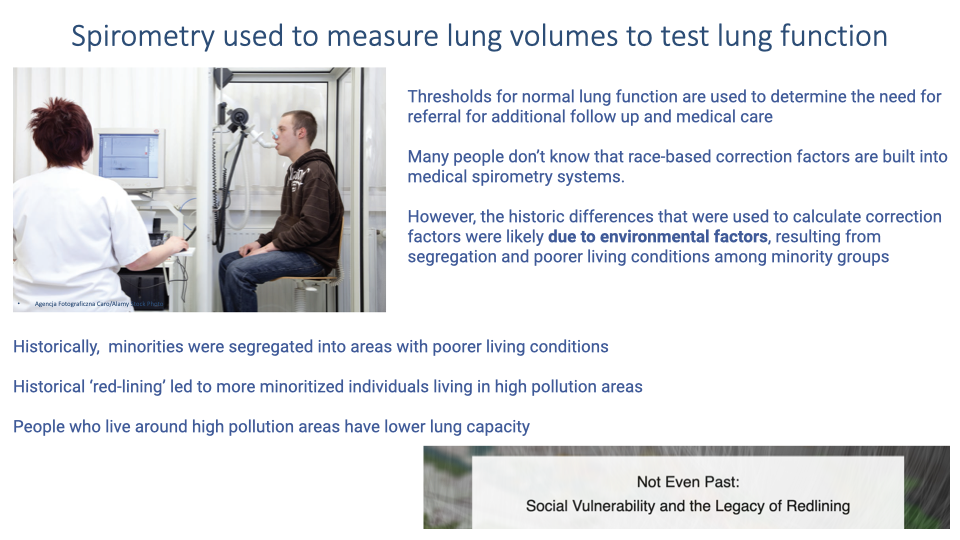
Race-based spirometry correction factors — A health equity issue
- Clinical spirometry systems use thresholds to determine whether lung function is normal and whether a patient should be referred for further care.
- Many systems include race-based correction factors developed decades ago, which apply different thresholds based on race under the assumption of inherent racial differences in lung capacity.
- Evidence suggests these differences are largely due to environmental factors, not inherent biology:
- Historical redlining concentrated minoritized communities in areas with higher pollution, less green space, and more industrial activity.
- These environmental exposures lead to higher rates of asthma and chronic lung disease.
- The legacy persists: people in historically redlined areas still show higher incidence of lung problems today.
- Using race-based thresholds can result in patients from minoritized groups needing worse lung function before being referred for treatment — perpetuating health disparities.
- This issue was highlighted during the COVID-19 pandemic and remains an active area of discussion in medicine.
Slide 27
Lecture 3 — Key takeaways
- The oxygen cascade describes the progressive drop in PO₂ from inspired air (~150 mmHg) to the mitochondria (~10–20 mmHg), with each step governed by specific physical equations.
- Vertebrate respiratory systems vary widely — mammalian tidal lungs have anatomical dead space, while fish gills and avian parabronchial lungs use unidirectional flow and have no dead space, making them more efficient.
- Breathing is driven by pressure differences created by the diaphragm and chest wall muscles, governed by Boyle’s Law. Airflow rate depends on both the pressure difference and airway resistance ($\dot{V} = \Delta P / R$).
- Dead space (anatomical + alveolar) reduces effective ventilation. Only alveolar ventilation ($\dot{V}_A = f_b \times (V_T - V_D)$) contributes to gas exchange.
- Spirometry measures lung volumes and ventilation rates, providing essential data for both clinical diagnosis and exercise physiology research.
Key Equations
| Equation | Name | Description |
|---|---|---|
| $P_IO_2 = F_IO_2 \times (P_{atm} - P_{H_2O})$ | Inspired PO₂ | Partial pressure of inspired O2, corrected for water vapor (47 mmHg at 37°C) |
| $P_2 = \frac{P_1 V_1}{V_2}$ | Boyle’s Law (applied) | Pressure change resulting from a change in lung volume during breathing |
| $\dot{V} = \frac{\Delta P}{R_{airway}}$ | Airflow equation | Volume flow rate of air equals the pressure difference divided by airway resistance |
| $\dot{V}_E = f_b \times V_T$ | Minute ventilation | Total rate of air movement in and out of the lungs per minute |
| $\dot{V}_A = f_b \times (V_T - V_D)$ | Alveolar ventilation rate | Rate of air reaching the gas exchange surfaces, accounting for dead space |
| $V_{D,\text{phys}} = V_{D,\text{alveolar}} + V_{D,\text{anatomic}}$ | Physiological dead space | Total dead space is the sum of anatomical and alveolar dead space |
| $\dot{V}O_2 = \dot{V}_A \times \beta_{gO_2} \times (P_IO_2 - P_EO_2)$ | Alveolar O2 delivery | Oxygen delivery rate to alveoli; in practice, measured using the Fick Principle |
Glossary of Key Terms
| Term | Definition |
|---|---|
| Oxygen supply cascade | The series of alternating convection and diffusion steps through which oxygen travels from the atmosphere to the mitochondria, with PO₂ decreasing at each stage. |
| Tidal ventilation | The pattern of breathing in which air flows in and out through the same airways, characteristic of mammalian lungs. |
| Anatomical dead space | The volume of the conducting airways (trachea, bronchi, bronchioles) that do not participate in gas exchange; approximately 150 mL in healthy adults. |
| Alveolar dead space | The volume of alveoli that are ventilated but not perfused with blood, and therefore do not contribute to gas exchange. |
| Physiological dead space | The total non-functional volume: anatomical dead space plus alveolar dead space. |
| Minute ventilation ($\dot{V}_E$) | The total volume of air moved in and out of the lungs per minute; also called pulmonary ventilation. |
| Alveolar ventilation ($\dot{V}_A$) | The volume of air per minute that actually reaches the alveolar gas exchange surfaces; equals minute ventilation minus dead space ventilation. |
| Conducting zone | The portion of the airways (generations 0–16) that transports air but does not participate in gas exchange. |
| Respiratory zone | The portion of the airways (generations 17–23) containing alveoli where gas exchange occurs by diffusion. |
| Diaphragm | The primary muscle of inspiration in mammals; its dome-shaped contraction increases thoracic volume in multiple dimensions. |
| Accessory muscles of ventilation | Muscles (sternocleidomastoid, scalenes, trapezius, pectoralis) that assist breathing during exercise or respiratory distress but are largely inactive during quiet breathing. |
| Airway resistance | The opposition to airflow through the airways, determined primarily by airway diameter. Increased in COPD, asthma, and other obstructive conditions. |
| Countercurrent exchange | A gas exchange arrangement (as in fish gills) where water and blood flow in opposite directions, maximizing O2 extraction. |
| Parabronchial lung | The avian lung structure in which air flows unidirectionally through rigid tubes (parabronchi), creating a cross-current exchange system with no dead space. |
| Spirometry | A clinical and research technique for measuring lung volumes and airflow rates by analyzing exhaled air. |
| Vital capacity | The maximum volume of air that can be exhaled after a maximum inhalation; equals IRV + VT + ERV. |
| Capacitance coefficient ($\beta_{gO_2}$) | A constant describing the amount of O2 that can be carried per unit volume of air per unit partial pressure difference. |